Development of the paediatric society of the African league against rheumatism (PAFLAR) JIA registry and clinical profile of JIA in Africa from the PAFLAR JIA registry.
Angela Nyangore Migowa, Wafa Hamdi, Soad Hashad, Hala Etayari, Awatif Abushhaiwia, Hanene Ferjani, Dorra Ben Nessib, Lobna Kharrat, Alia Fazaa, Lawrence Owino, Ayodele Faleye, Sheila Agyeiwaa Owusu, Doaa Mosad Mosa, Mervat Eissa, Samah Ismail Nasef, Gehad Gamal Elsehrawy, Rachel Odhiambo, James Orwa, Mohammed Hassan Abu-Zaid
{"title":"Development of the paediatric society of the African league against rheumatism (PAFLAR) JIA registry and clinical profile of JIA in Africa from the PAFLAR JIA registry.","authors":"Angela Nyangore Migowa, Wafa Hamdi, Soad Hashad, Hala Etayari, Awatif Abushhaiwia, Hanene Ferjani, Dorra Ben Nessib, Lobna Kharrat, Alia Fazaa, Lawrence Owino, Ayodele Faleye, Sheila Agyeiwaa Owusu, Doaa Mosad Mosa, Mervat Eissa, Samah Ismail Nasef, Gehad Gamal Elsehrawy, Rachel Odhiambo, James Orwa, Mohammed Hassan Abu-Zaid","doi":"10.1186/s12969-024-01000-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The spectrum of Juvenile Idiopathic Arthritis (JIA) in Africa is still largely unknown. We thus set out to illustrate how we set up the PAFLAR JIA registry and describe the clinical profile of Juvenile Idiopathic Arthritis across various regions in Africa.</p><p><strong>Methods: </strong>We carried out a retrospective observational cohort study where collaborators were trained on use of the existing PAFLAR REDCAP database to enter data for the JIA patients currently under their care capturing their epidemiological data, clinical features, laboratory investigations, diagnosis and therapy at initial diagnosis. Descriptive statistics including means, standard deviations, medians, interquartile ranges (IQR) for continuous variables and proportions for categorical variables were calculated as appropriate. Tests for difference between groups were performed between categorical variables using Pearson's chi-square or Fisher's exact tests. All analyses were performed using SPSS version 22 software.</p><p><strong>Results: </strong>We enrolled 302 patients, 58.6% (177 of 302) of whom were female. The median age of disease onset was 7 years (range 3-11 years) and the median age at diagnosis was 8.5 years (range 5-12 years). The median duration delay in diagnosis was 6 months (range 1-20.8 months). The JIA categories included Systemic JIA 18.9% (57), Oligoarticular JIA 19.2% (83), Polyarticular RF + ve 5% (15), Polyarticular RF-ve 17.9% (54), Enthesitis Related Arthritis (ERA) 18.2% (55), Psoriatic Arthritis 7% (21) and undifferentiated JIA 5.6% (17). As regards treatment the commonest therapies were NSAID therapy at 31.1%, synthetic DMARDs at 18.1%, synthetic DMARDs combined with NSAIDs at 17.5% and steroid therapy at 9.6%. Biological DMARDs accounted for 2.3% of therapies offered to our patients at diagnosis. The average JADAS score was 10.3 (range 4.8-18.2) and the average CHAQ score was 1.3 (range 0.7-2.0).</p><p><strong>Conclusion: </strong>Our study highlights strategies involved in setting up a Pan-African paediatric rheumatology registry that embraces our broad diversity and the vast spectrum of JIA in Africa while comparing the various therapies available to our patients. The PAFLAR JIA registry strives to ensure a comprehensive representation of the diverse healthcare landscapes within the continent. Further longitudinal observation studies are required to ascertain the long-term outcomes of our patients and ultimately help inform policy to create a more favorable health ecosystem to support the healthcare needs of JIA patients in Africa.</p>","PeriodicalId":54630,"journal":{"name":"Pediatric Rheumatology","volume":"22 1","pages":"67"},"PeriodicalIF":2.3000,"publicationDate":"2024-07-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11264440/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Rheumatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12969-024-01000-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The spectrum of Juvenile Idiopathic Arthritis (JIA) in Africa is still largely unknown. We thus set out to illustrate how we set up the PAFLAR JIA registry and describe the clinical profile of Juvenile Idiopathic Arthritis across various regions in Africa.
Methods: We carried out a retrospective observational cohort study where collaborators were trained on use of the existing PAFLAR REDCAP database to enter data for the JIA patients currently under their care capturing their epidemiological data, clinical features, laboratory investigations, diagnosis and therapy at initial diagnosis. Descriptive statistics including means, standard deviations, medians, interquartile ranges (IQR) for continuous variables and proportions for categorical variables were calculated as appropriate. Tests for difference between groups were performed between categorical variables using Pearson's chi-square or Fisher's exact tests. All analyses were performed using SPSS version 22 software.
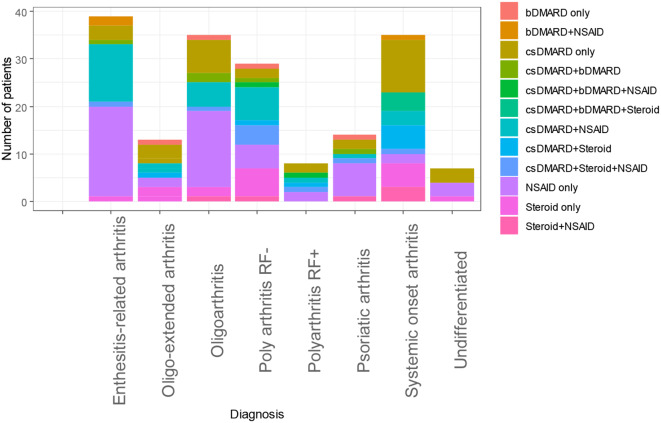
Results: We enrolled 302 patients, 58.6% (177 of 302) of whom were female. The median age of disease onset was 7 years (range 3-11 years) and the median age at diagnosis was 8.5 years (range 5-12 years). The median duration delay in diagnosis was 6 months (range 1-20.8 months). The JIA categories included Systemic JIA 18.9% (57), Oligoarticular JIA 19.2% (83), Polyarticular RF + ve 5% (15), Polyarticular RF-ve 17.9% (54), Enthesitis Related Arthritis (ERA) 18.2% (55), Psoriatic Arthritis 7% (21) and undifferentiated JIA 5.6% (17). As regards treatment the commonest therapies were NSAID therapy at 31.1%, synthetic DMARDs at 18.1%, synthetic DMARDs combined with NSAIDs at 17.5% and steroid therapy at 9.6%. Biological DMARDs accounted for 2.3% of therapies offered to our patients at diagnosis. The average JADAS score was 10.3 (range 4.8-18.2) and the average CHAQ score was 1.3 (range 0.7-2.0).
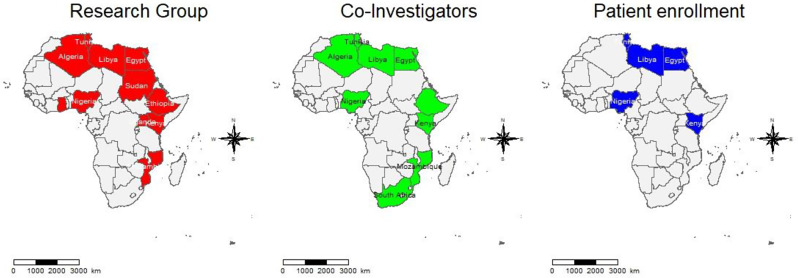
Conclusion: Our study highlights strategies involved in setting up a Pan-African paediatric rheumatology registry that embraces our broad diversity and the vast spectrum of JIA in Africa while comparing the various therapies available to our patients. The PAFLAR JIA registry strives to ensure a comprehensive representation of the diverse healthcare landscapes within the continent. Further longitudinal observation studies are required to ascertain the long-term outcomes of our patients and ultimately help inform policy to create a more favorable health ecosystem to support the healthcare needs of JIA patients in Africa.
期刊介绍:
Pediatric Rheumatology is an open access, peer-reviewed, online journal encompassing all aspects of clinical and basic research related to pediatric rheumatology and allied subjects.
The journal’s scope of diseases and syndromes include musculoskeletal pain syndromes, rheumatic fever and post-streptococcal syndromes, juvenile idiopathic arthritis, systemic lupus erythematosus, juvenile dermatomyositis, local and systemic scleroderma, Kawasaki disease, Henoch-Schonlein purpura and other vasculitides, sarcoidosis, inherited musculoskeletal syndromes, autoinflammatory syndromes, and others.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
