{"title":"Laser lithotripsy with balloon enteroscopy-assisted peroral cholangioscopy for a large common bile duct stone after Billroth II gastrectomy","authors":"Haruo Miwa, Kazuya Sugimori, Shin Maeda","doi":"10.1111/den.14888","DOIUrl":null,"url":null,"abstract":"<p>Endoscopic procedures for large common bile duct stones in patients with altered anatomy remain challenging, despite reports on direct peroral cholangioscopy (POCS).<span><sup>1-4</sup></span> Recently, a novel slim cholangioscope (9F eyeMAX; Micro-Tech, Nanjing, China) facilitated balloon enteroscopy-assisted POCS (BE-POCS).<span><sup>5</sup></span></p><p>An 83-year-old man, after Billroth II gastrectomy, was admitted with a large common bile duct stone. BE-POCS using a Holmium YAG (Ho:YAG) laser was employed for stone removal (Video S1). A balloon enteroscope (SIF-H290S; Olympus, Tokyo, Japan) was inserted into the afferent loop, and cholangiography revealed a large stone (15 mm) in the dilated common bile duct (20 mm). After papillary balloon dilation (15 mm), 9F eyeMAX was smoothly inserted via enteroscopy. A large stone was located in the hepatic hilum. Ho:YAG laser (LithoEVO; EDAP TMS, Lyon, France) lithotripsy effectively crushed the stone core under cholangioscope guidance (Fig. 1). The irrigation ability was sufficient to maintain a clear view because of a separate irrigation channel. A basket catheter (LithoCrush V; Olympus) was used to remove the fragments; however, the largest piece could not be extracted, and mechanical lithotripsy failed. A plastic stent was placed until the second session because of the procedure length (100 min). One month later, the largest fragment was completely crushed using the Ho: YAG laser to prevent basket impaction (Fig. 2). The green color of the laser helped detect the probe tip during the procedure. The fragmented stones were removed using a spiral basket catheter (KANEKA Medics, Tokyo, Japan). Cholangioscopy confirmed no residual stones in the intrahepatic bile ducts. Finally, small fragments were extracted using a microbasket catheter (ABIS, Hyogo, Japan) (60 min).</p><p>This is the first report of laser lithotripsy with BE-POCS for a patient with Billroth II gastrectomy. Ho:YAG laser lithotripsy using a slim cholangioscope is useful for treating difficult stones in patients with altered anatomy.</p><p>Authors declare no conflict of interest for this article.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 9","pages":"1059-1061"},"PeriodicalIF":4.7000,"publicationDate":"2024-07-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14888","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14888","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Endoscopic procedures for large common bile duct stones in patients with altered anatomy remain challenging, despite reports on direct peroral cholangioscopy (POCS).1-4 Recently, a novel slim cholangioscope (9F eyeMAX; Micro-Tech, Nanjing, China) facilitated balloon enteroscopy-assisted POCS (BE-POCS).5
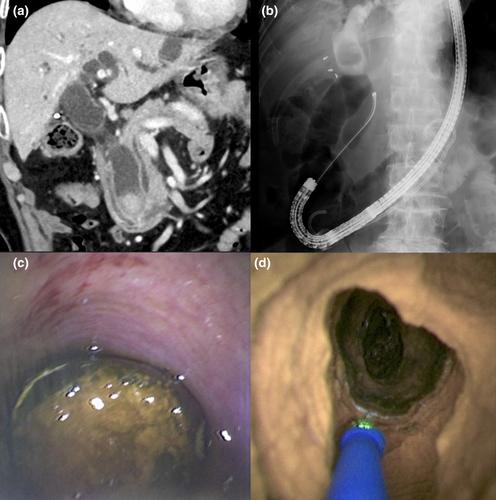
An 83-year-old man, after Billroth II gastrectomy, was admitted with a large common bile duct stone. BE-POCS using a Holmium YAG (Ho:YAG) laser was employed for stone removal (Video S1). A balloon enteroscope (SIF-H290S; Olympus, Tokyo, Japan) was inserted into the afferent loop, and cholangiography revealed a large stone (15 mm) in the dilated common bile duct (20 mm). After papillary balloon dilation (15 mm), 9F eyeMAX was smoothly inserted via enteroscopy. A large stone was located in the hepatic hilum. Ho:YAG laser (LithoEVO; EDAP TMS, Lyon, France) lithotripsy effectively crushed the stone core under cholangioscope guidance (Fig. 1). The irrigation ability was sufficient to maintain a clear view because of a separate irrigation channel. A basket catheter (LithoCrush V; Olympus) was used to remove the fragments; however, the largest piece could not be extracted, and mechanical lithotripsy failed. A plastic stent was placed until the second session because of the procedure length (100 min). One month later, the largest fragment was completely crushed using the Ho: YAG laser to prevent basket impaction (Fig. 2). The green color of the laser helped detect the probe tip during the procedure. The fragmented stones were removed using a spiral basket catheter (KANEKA Medics, Tokyo, Japan). Cholangioscopy confirmed no residual stones in the intrahepatic bile ducts. Finally, small fragments were extracted using a microbasket catheter (ABIS, Hyogo, Japan) (60 min).
This is the first report of laser lithotripsy with BE-POCS for a patient with Billroth II gastrectomy. Ho:YAG laser lithotripsy using a slim cholangioscope is useful for treating difficult stones in patients with altered anatomy.
Authors declare no conflict of interest for this article.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
