Ahmed Alasker, Turki Rashed Alnafisah, Areez Shafqat, Belal Nedal Sabbah, Marwan Alaswad, Mohammad Alghafees, Abdullah Alhaider, Abdulrahman Alsayyari, Naif Althonayan, Mohammed Al-Otaibi, Salman Bin Ofisan, Mohammed Ghazi Alharbi, Bader Alsaikhan, Abdullah Al-Khayal
{"title":"Nephrectomies in Saudi Arabia: A Comprehensive Analysis of Outcomes from a High-Volume Minimally Invasive Surgery Center.","authors":"Ahmed Alasker, Turki Rashed Alnafisah, Areez Shafqat, Belal Nedal Sabbah, Marwan Alaswad, Mohammad Alghafees, Abdullah Alhaider, Abdulrahman Alsayyari, Naif Althonayan, Mohammed Al-Otaibi, Salman Bin Ofisan, Mohammed Ghazi Alharbi, Bader Alsaikhan, Abdullah Al-Khayal","doi":"10.15586/jkcvhl.v11i3.332","DOIUrl":null,"url":null,"abstract":"<p><p>Literature reporting on the outcomes of the different procedures of nephrectomies (open vs laparoscopic vs robotic) in Saudi Arabia remains limited. Compare surgical and oncological outcomes between open and minimally invasive nephrectomies. A retrospective cohort study. The present study included all adult patients who underwent nephrectomies between January 1, 2015 and January 31, 2023. We collected demographic, preoperative, intraoperative, and postoperative data on 408 adult cancer patients who underwent nephrectomies at our center between January 2015 and January 2023. Statistical differences were calculated between procedure types. Overall survival was calculated using Kaplan-Meier curves with log-rank tests. P<0.05 was considered statistically significant. Measures of operative success (intraoperative blood loss, intraoperative and postoperative complications, and hospital stay) and oncological outcomes (local recurrence, metastatic progression, and chemotherapy use) between different procedure and nephrectomy types for cancer patients. A total of 408 cancer patients underwent nephrectomies. In cancer patients, open nephrectomy was associated with significantly higher intraoperative blood loss (p<0.001), incidence of blood transfusions (p<0.001), hospital stay (p<0.001), intraoperative complications (p=0.027 and p=0.001, respectively), local recurrence (p<0.001), metastatic progression (p=0.001), and chemotherapy (p=0.001) than minimally invasive surgery, but survival differences across procedure types were not statistically significant (log-rank p-value = 0.054). Regarding nephrectomy type, significant differences were observed in tumor size (p < 0.001), initial procedure type (p<0.001), operation time (p<0.001), blood transfusion (p=0.033), length of hospital stay (p=0.004), intraoperative complications (p=0.020), postoperative complications (p=0.025), Clavien classification (p=0.003), mortality (p=0.022), metastatic progression (p<0.001), and chemotherapy use (p=0.001) between simple/total nephrectomy, radical nephrectomy (RN), partial nephrectomy (PN), and nephroureterectomy. Survival differences between the four nephrectomy types were statistically significant (log-rank p value = 0.001). Minimally invasive nephrectomies reduce inpatient morbidity while conferring equivalent oncological and surgical outcomes.</p>","PeriodicalId":44291,"journal":{"name":"Journal of Kidney Cancer and VHL","volume":"11 3","pages":"1-12"},"PeriodicalIF":1.9000,"publicationDate":"2024-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11261389/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Kidney Cancer and VHL","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15586/jkcvhl.v11i3.332","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
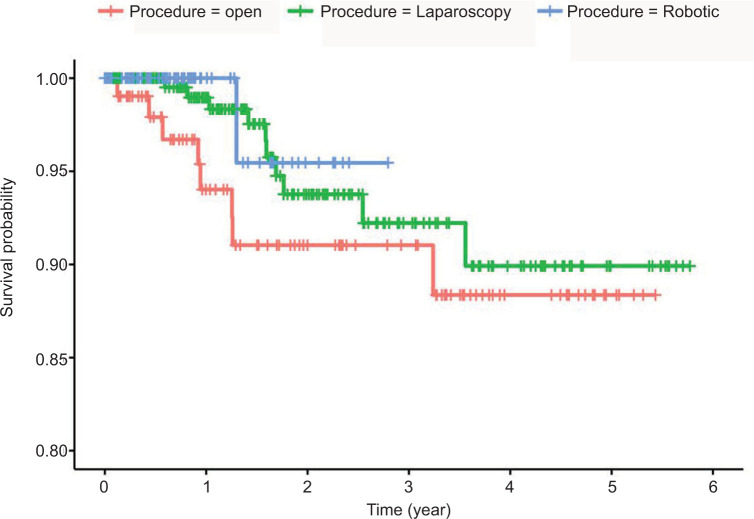
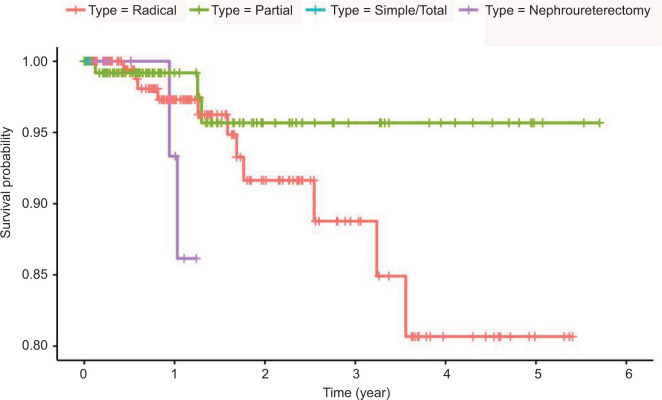
Literature reporting on the outcomes of the different procedures of nephrectomies (open vs laparoscopic vs robotic) in Saudi Arabia remains limited. Compare surgical and oncological outcomes between open and minimally invasive nephrectomies. A retrospective cohort study. The present study included all adult patients who underwent nephrectomies between January 1, 2015 and January 31, 2023. We collected demographic, preoperative, intraoperative, and postoperative data on 408 adult cancer patients who underwent nephrectomies at our center between January 2015 and January 2023. Statistical differences were calculated between procedure types. Overall survival was calculated using Kaplan-Meier curves with log-rank tests. P<0.05 was considered statistically significant. Measures of operative success (intraoperative blood loss, intraoperative and postoperative complications, and hospital stay) and oncological outcomes (local recurrence, metastatic progression, and chemotherapy use) between different procedure and nephrectomy types for cancer patients. A total of 408 cancer patients underwent nephrectomies. In cancer patients, open nephrectomy was associated with significantly higher intraoperative blood loss (p<0.001), incidence of blood transfusions (p<0.001), hospital stay (p<0.001), intraoperative complications (p=0.027 and p=0.001, respectively), local recurrence (p<0.001), metastatic progression (p=0.001), and chemotherapy (p=0.001) than minimally invasive surgery, but survival differences across procedure types were not statistically significant (log-rank p-value = 0.054). Regarding nephrectomy type, significant differences were observed in tumor size (p < 0.001), initial procedure type (p<0.001), operation time (p<0.001), blood transfusion (p=0.033), length of hospital stay (p=0.004), intraoperative complications (p=0.020), postoperative complications (p=0.025), Clavien classification (p=0.003), mortality (p=0.022), metastatic progression (p<0.001), and chemotherapy use (p=0.001) between simple/total nephrectomy, radical nephrectomy (RN), partial nephrectomy (PN), and nephroureterectomy. Survival differences between the four nephrectomy types were statistically significant (log-rank p value = 0.001). Minimally invasive nephrectomies reduce inpatient morbidity while conferring equivalent oncological and surgical outcomes.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
