Acute lymphoblastic leukemia (ALL) is one of the most common malignancies among children. Despite success in frontline treatment, 20% of children will relapse or show resistance to treatment.
The aim of this study is to evaluate the clinical characteristics of children diagnosed and treated for refractory or relapsed ALL and determine 3-year overall survival (OS) outcomes.
This study involved a retrospective chart review of patients aged 1–14 years diagnosed with ALL during January 2002 to December 2018. Data were extracted for baseline characteristics at diagnosis and at relapse.
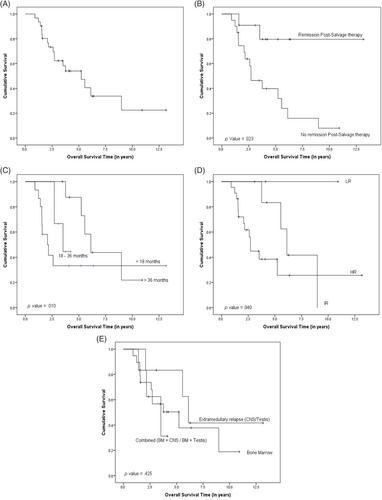
A total of 347 newly diagnosed children with ALL were identified, among whom there were three induction failures (IF) and 28 relapses, resulting in a cohort of 31 patients with a relapse rate of 9%. The male-to-female ratio was 4.16:1, and the mean duration of first complete remission (CR1) was 26 months. Fifteen (48%) patients relapsed ≤18 months, 7 (23%) during 18–36 months, and 9 (29%) relapsed >36 months of IF or CR1. Nineteen patients (61%) had isolated bone marrow (BM) relapse, 7 (23%) patients experienced isolated extramedullary relapse (5 isolated CNS relapse and 2 isolated testicular relapse), and 5 (16%) patients experienced BM involvement with other sites (4 BM + CNS and 1 BM + testis). The 3-year OS of the cohort was 62.3%, while in patients with CR post first-salvage therapy, a 3-year OS of 79.5% was observed (p value <.05 compared with patients who did not achieve remission post first-salvage therapy, 3-year OS: 46.4%). The same statistical difference was observed in 3-year OS when comparing the duration of remission of CR prior to relapse: ≤18 months, 33.2%; 18–36 months, 66.7%; and >36 months, 87.5%. The same trend continued when comparing 3-year OS based on risk stratification at relapse: low risk (LR), 83.3%; intermediate risk (IR), 80%; and high risk (HR), 44.8%.
The incidence and outcomes reported are comparable to internationally reported data regarding the duration of CR1. Risk stratification at relapse and remission status post-salvage therapy were identified as significant prognostic factors for survival. No survival difference was observed among patients who received hematopoietic stem cell transplantation after induction compared with those who received chemotherapy, which could be attributed to the smaller sample size, warranting a multi-institutional observational study. These findings corroborate the need for novel therapies and treatment approaches.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
