Preoperative forced expiratory volume in one second and postoperative respiratory outcomes in nonpulmonary and noncardiac surgery: a retrospective cohort study.
{"title":"Preoperative forced expiratory volume in one second and postoperative respiratory outcomes in nonpulmonary and noncardiac surgery: a retrospective cohort study.","authors":"Toshiyuki Mizota, Miho Hamada, Akiko Hirotsu, Li Dong, Shino Matsukawa, Chikashi Takeda, Moritoki Egi","doi":"10.1186/s40981-024-00729-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although the usefulness of pulmonary function tests has been established for lung resection and coronary artery bypass surgeries, the association between preoperative pulmonary function test and postoperative respiratory complications in nonpulmonary and noncardiac surgery is inconclusive. The purpose of this study was to determine the association between preoperative forced expiratory volume in one second (FEV1) on pulmonary function test and the development of postoperative respiratory failure and/or death in patients undergoing major nonpulmonary and noncardiac surgery.</p><p><strong>Methods: </strong>Adult patients aged ≥ 18 years and who underwent nonpulmonary and noncardiac surgery with expected moderate to high risk of perioperative complications from June 2012 to March 2019 were included. The primary exposure was preoperative FEV1 measured by pulmonary function test within six months before surgery. The primary outcome was respiratory failure (i.e., invasive positive pressure ventilation for at least 24 h after surgery or reintubation) and/or death within 30 days after surgery. A logistic regression model was used to adjust for the respiratory failure risk index, which is a scoring system that predicts the probability of postoperative respiratory failure based on patient and surgical factors, and to examine the association between preoperative FEV1 and the development of postoperative respiratory failure and/or death.</p><p><strong>Results: </strong>Respiratory failure and/or death occurred within 30 days after surgery in 52 (0.9%) of 5562 participants. The incidence of respiratory failure and/or death in patients with FEV1 ≥ 80%, 70%- < 80%, 60%- < 70%, and < 60% was 0.9%, 0.6%, 1.7%, and 1.2%, respectively. Multivariable logistic regression analysis showed no significant association between preoperative FEV1 and postoperative respiratory failure and/or death (adjusted odds ratio per 10% decrease in FEV1: 1.01, 95% confidence interval: 0.88-1.17, P = 0.838). Addition of FEV1 information to the respiratory failure risk index did not improve the prediction of respiratory failure and/or death [area under the receiver operating characteristics curve: 0.78 (95% confidence interval: 0.72-0.84) and 0.78 (95% confidence interval: 0.72-0.84), respectively; P = 0.84].</p><p><strong>Conclusion: </strong>We found no association between preoperative FEV1 and postoperative respiratory failure and/or death in patients undergoing major nonpulmonary and noncardiac surgery.</p>","PeriodicalId":14635,"journal":{"name":"JA Clinical Reports","volume":"10 1","pages":"44"},"PeriodicalIF":1.0000,"publicationDate":"2024-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11272759/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JA Clinical Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40981-024-00729-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Although the usefulness of pulmonary function tests has been established for lung resection and coronary artery bypass surgeries, the association between preoperative pulmonary function test and postoperative respiratory complications in nonpulmonary and noncardiac surgery is inconclusive. The purpose of this study was to determine the association between preoperative forced expiratory volume in one second (FEV1) on pulmonary function test and the development of postoperative respiratory failure and/or death in patients undergoing major nonpulmonary and noncardiac surgery.
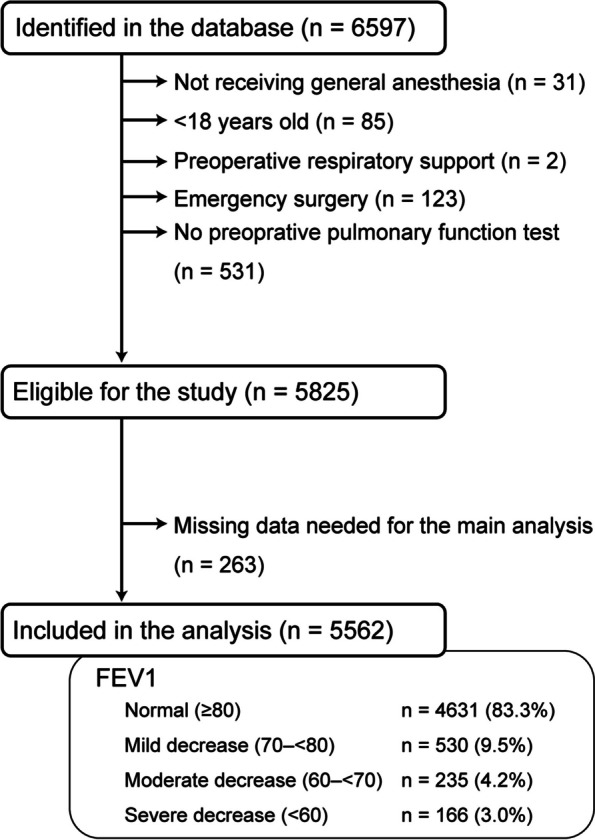
Methods: Adult patients aged ≥ 18 years and who underwent nonpulmonary and noncardiac surgery with expected moderate to high risk of perioperative complications from June 2012 to March 2019 were included. The primary exposure was preoperative FEV1 measured by pulmonary function test within six months before surgery. The primary outcome was respiratory failure (i.e., invasive positive pressure ventilation for at least 24 h after surgery or reintubation) and/or death within 30 days after surgery. A logistic regression model was used to adjust for the respiratory failure risk index, which is a scoring system that predicts the probability of postoperative respiratory failure based on patient and surgical factors, and to examine the association between preoperative FEV1 and the development of postoperative respiratory failure and/or death.
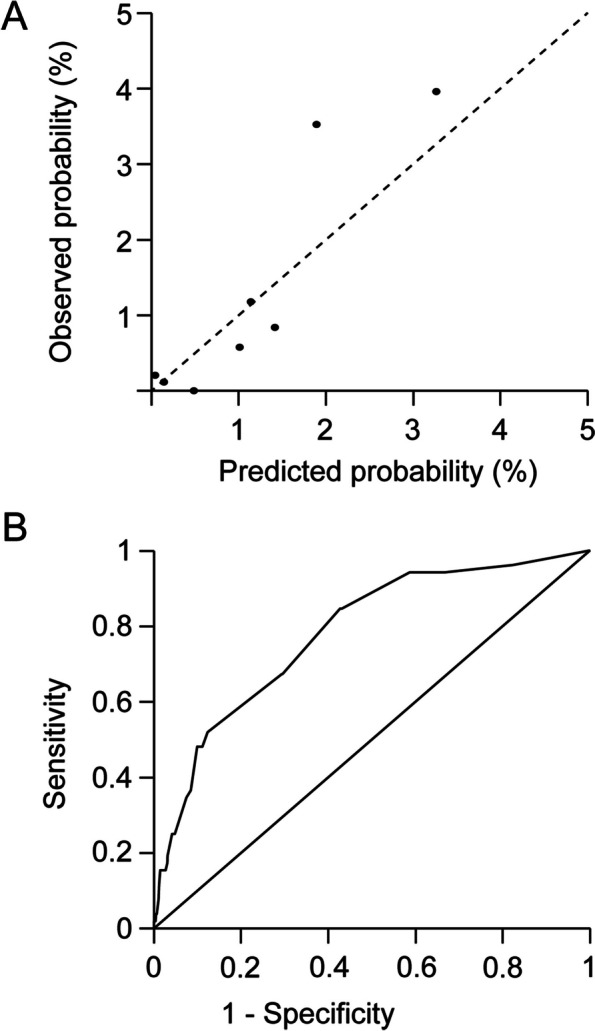
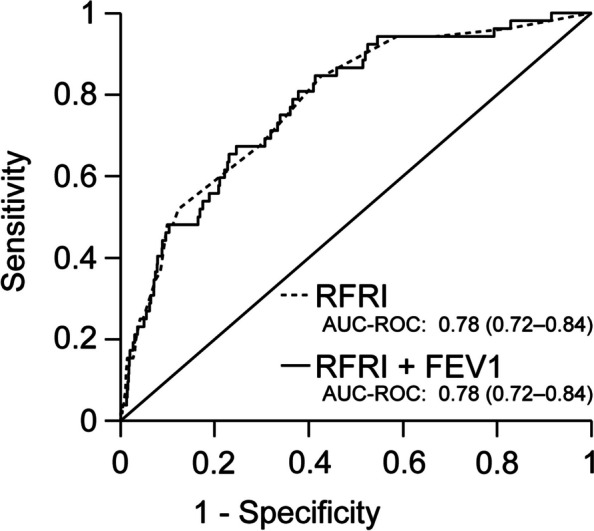
Results: Respiratory failure and/or death occurred within 30 days after surgery in 52 (0.9%) of 5562 participants. The incidence of respiratory failure and/or death in patients with FEV1 ≥ 80%, 70%- < 80%, 60%- < 70%, and < 60% was 0.9%, 0.6%, 1.7%, and 1.2%, respectively. Multivariable logistic regression analysis showed no significant association between preoperative FEV1 and postoperative respiratory failure and/or death (adjusted odds ratio per 10% decrease in FEV1: 1.01, 95% confidence interval: 0.88-1.17, P = 0.838). Addition of FEV1 information to the respiratory failure risk index did not improve the prediction of respiratory failure and/or death [area under the receiver operating characteristics curve: 0.78 (95% confidence interval: 0.72-0.84) and 0.78 (95% confidence interval: 0.72-0.84), respectively; P = 0.84].
Conclusion: We found no association between preoperative FEV1 and postoperative respiratory failure and/or death in patients undergoing major nonpulmonary and noncardiac surgery.
期刊介绍:
JA Clinical Reports is a companion journal to the Journal of Anesthesia (JA), the official journal of the Japanese Society of Anesthesiologists (JSA). This journal is an open access, peer-reviewed, online journal related to clinical anesthesia practices such as anesthesia management, pain management and intensive care. Case reports are very important articles from the viewpoint of education and the cultivation of scientific thinking in the field of anesthesia. However, submissions of anesthesia research and clinical reports from Japan are notably decreasing in major anesthesia journals. Therefore, the JSA has decided to launch a new journal, JA Clinical Reports, to encourage JSA members, particularly junior Japanese anesthesiologists, to publish papers in English language.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
