{"title":"Endoscopic transpapillary drainage through the pancreatic stump for postoperative pancreatic fistula after distal pancreatectomy","authors":"Takafumi Mie, Takashi Sasaki, Naoki Sasahira","doi":"10.1111/den.14894","DOIUrl":null,"url":null,"abstract":"<p>Postoperative pancreatic fistula (POPF) is one of the major complications following distal pancreatectomy (DP). With the increasing adoption of laparoscopic and robotic approaches, the rate of clinically relevant POPF is reported as between 18.2–26.7%.<span><sup>1, 2</sup></span> When POPF does not improve with conservative treatment, interventions such as percutaneous drainage (PTD), endoscopic ultrasound-guided transluminal drainage (EUS-TD), and endoscopic transpapillary drainage (ETPD) are employed.<span><sup>3-5</sup></span> However, PTD and EUS-TD may not always be appropriate due to interfering blood vessels, the distance from the abdominal or gastrointestinal wall to the POPF, or an immature POPF wall. On the other hand, while ETPD may reduce leakage of pancreatic fluid from the main pancreatic duct into the POPF, it may sometimes be ineffective due to indirect drainage of the POPF.</p><p>For such cases, we performed ETPD through the pancreatic duct stump (PDS). A 59-year-old man developed POPF with fever and abdominal pain 23 days after DP. Pancreatography from near the PDS was performed to confirm the leakage into the POPF, followed by guidewire insertion into the POPF. An endoscopic nasopancreatic drainage (ENPD) tube was subsequently placed into the POPF. After confirming the shrinkage of POPF in 1–2 weeks, the ENPD tube was replaced with a pancreatic duct stent, without penetrating the PDS (Video S1). The ENPD tube over the PDS enabled direct drainage of the POPF, and the pancreatic duct stent could relieve the intrapancreatic high pressure because of Oddi.<span><sup>4</sup></span> The stent was removed a few months later after confirming the absence of POPF recurrence by computed tomography (Fig. 1). This strategy was applied in four cases, with no cases with recurrent POPF (Table 1). This method provides an alternative option for PTD or EUS-TD, especially when the POPF has distance from the abdominal or gastrointestinal wall, or when the POPF wall is immature in the early postoperative period.</p><p>Authors declare no conflict of interest for this article.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 10","pages":"1176-1178"},"PeriodicalIF":4.7000,"publicationDate":"2024-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14894","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14894","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Postoperative pancreatic fistula (POPF) is one of the major complications following distal pancreatectomy (DP). With the increasing adoption of laparoscopic and robotic approaches, the rate of clinically relevant POPF is reported as between 18.2–26.7%.1, 2 When POPF does not improve with conservative treatment, interventions such as percutaneous drainage (PTD), endoscopic ultrasound-guided transluminal drainage (EUS-TD), and endoscopic transpapillary drainage (ETPD) are employed.3-5 However, PTD and EUS-TD may not always be appropriate due to interfering blood vessels, the distance from the abdominal or gastrointestinal wall to the POPF, or an immature POPF wall. On the other hand, while ETPD may reduce leakage of pancreatic fluid from the main pancreatic duct into the POPF, it may sometimes be ineffective due to indirect drainage of the POPF.
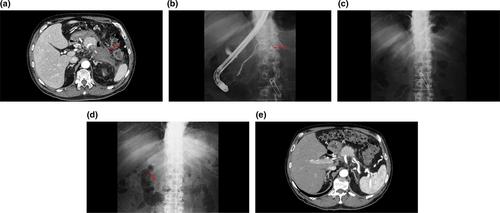
For such cases, we performed ETPD through the pancreatic duct stump (PDS). A 59-year-old man developed POPF with fever and abdominal pain 23 days after DP. Pancreatography from near the PDS was performed to confirm the leakage into the POPF, followed by guidewire insertion into the POPF. An endoscopic nasopancreatic drainage (ENPD) tube was subsequently placed into the POPF. After confirming the shrinkage of POPF in 1–2 weeks, the ENPD tube was replaced with a pancreatic duct stent, without penetrating the PDS (Video S1). The ENPD tube over the PDS enabled direct drainage of the POPF, and the pancreatic duct stent could relieve the intrapancreatic high pressure because of Oddi.4 The stent was removed a few months later after confirming the absence of POPF recurrence by computed tomography (Fig. 1). This strategy was applied in four cases, with no cases with recurrent POPF (Table 1). This method provides an alternative option for PTD or EUS-TD, especially when the POPF has distance from the abdominal or gastrointestinal wall, or when the POPF wall is immature in the early postoperative period.
Authors declare no conflict of interest for this article.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
