Marion Denos PhD, Ernest Obeng Asante MSc, Rannveig Sakshaug Eldholm MD, PhD, Geir Selbæk MD, PhD, Håvard Kjesbu Skjellegrind MD, PhD, Xiao-Mei Mai MD, PhD, Yue Chen MD, PhD, Yi-Qian Sun MD, PhD
{"title":"The association between clinically evaluated cognitive function and oral health in Norwegian older adults: The HUNT Study","authors":"Marion Denos PhD, Ernest Obeng Asante MSc, Rannveig Sakshaug Eldholm MD, PhD, Geir Selbæk MD, PhD, Håvard Kjesbu Skjellegrind MD, PhD, Xiao-Mei Mai MD, PhD, Yue Chen MD, PhD, Yi-Qian Sun MD, PhD","doi":"10.1111/jgs.19103","DOIUrl":null,"url":null,"abstract":"<p>Poor oral health and neurocognitive disorders (NCDs) are both important public health challenges in the general older population.<span><sup>1, 2</sup></span> Older adults with NCDs may have poorer oral health due to decline in self-care, medication side effects, and lower dietary quality.<span><sup>3</sup></span> Yet, the association between cognitive function and oral health is unclear.<span><sup>4</sup></span> Wu et al. advocated a standardized assessment of oral health and cognitive states to better evaluate their potential associations.<span><sup>4</sup></span></p><p>The aim of this cross-sectional study was to explore the relationship between cognitive function and oral health, both thoroughly assessed by clinical experts, in a home-dwelling Norwegian older adult population.</p><p>Our study population, derived from the Trøndelag Health Study Survey 4 (HUNT4), included 633 participants aged 70 years or older who attended both the HUNT4 Oral Health Study and HUNT4 70+.<span><sup>5-7</sup></span></p><p>Clinical experts assessed the cognitive function of HUNT4 70+ participants after a comprehensive clinical evaluation, following the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria.<span><sup>7</sup></span> In the current study, mild cognitive impairment (MCI) and dementia were diagnosed and collectively categorized as NCDs.</p><p>Participants in the HUNT4 Oral Health Study underwent clinical and radiographic examinations conducted by trained and calibrated dentists. Decayed, missing, and filled teeth (DMFT) were calculated using the clinical and radiographic caries registration of dental status.<span><sup>5</sup></span> Decayed teeth were caries lesions confined in dentine (grades 3–5), secondary caries in dentine, and root caries with cavitation. Severe periodontitis was defined as periodontal Stage 3 or 4 based on radiographic bone loss and periodontal stage assessments.<span><sup>6</sup></span></p><p>The relationships between cognitive function and the number of decayed teeth, DMFT or natural teeth were assessed using negative binomial regression models, computing ratios of means (RMs) with 95% confidence intervals (CIs). The relationship between cognitive function and the prevalence of severe periodontitis was estimated using Poisson regression with robust error variance, providing prevalence ratios (PRs) with 95% CIs. Covariates such as age, sex, education, marital status, body mass index (BMI), smoking status, and alcohol consumption were considered potential confounders based on the literature.<span><sup>4, 8, 9</sup></span> All statistical analyses were performed with STATA/MP 18.</p><p>Table 1 describes the baseline characteristics of the study population overall and by cognitive function (normal and NCDs). As shown in Figure 1A, the mean number of decayed teeth was higher for participants with NCDs compared to those with normal cognitive function (1.8 vs. 1.5). NCDs were associated with a 19% increase in the mean number of decayed teeth in the adjusted model (RM 1.19, 95% CI 0.98–1.46), although it was not statistically significant (<i>p</i>-value = 0.09). It appears that a dose–response association was demonstrated (<i>p</i>-value for trend = 0.09): participants with MCI had an 18% increase (RM 1.18, 95% CI 0.95–1.47) in the mean number of decayed teeth, while those with dementia had a 25% increase (RM 1.25, 95% CI 0.84–1.86). There was no association between NCDs and the number of DMFT (Supplementary Table S1). Participants with dementia had a 9% decrease in the mean number of natural teeth compared to those with normal cognitive function (RM 0.91, 95% CI 0.84–0.99, Supplementary Table S2). The prevalence of severe periodontitis was similar among participants with NCDs compared to those with normal cognitive function (Figure 1B: PR 1.02, 95% CI 0.85–1.21).</p><p>Few studies have explored the relationships between cognitive function and clinically measured oral health components. The available measures were often limited to self-rated oral health, questionnaires, or non-dental screening tool.<span><sup>4, 8, 10</sup></span> Our findings support the previous studies that reported an association between cognitive function and self-reported oral health.<span><sup>8, 10</sup></span> Our study, along with previous research,<span><sup>10</sup></span> suggests that poor cognitive function may lead to neglected self-care, resulting in poorer oral hygiene and oral health in older people.</p><p>The current study is one of the first to investigate potential associations between cognitive function and detailed oral health components, both clinically evaluated. NCDs were diagnosed by clinical experts, and oral health evaluation was thoroughly conducted by trained specialists in dentistry, which makes this study unique.<span><sup>5-7</sup></span> However, the sample size was small, leading to relatively imprecise estimates with wider 95% CIs.</p><p>In conclusion, our results suggested that older adults with NCDs had a higher number of dental caries than those with normal cognitive function, and participants with dementia had fewer natural teeth. This highlights the need to improve the oral health care of home-dwelling older adults with NCDs.</p><p>MD wrote the initial draft of the manuscript. XMM and YQS performed the literature search and contributed to the study design. GS, HKS, and YQS were responsible for data collection. MD, EOA, and YQS conducted statistical analyses and interpreted results. MD, EOA, RSE, GS, HKS, XMM, YC, and YQS participated in the data interpretation and the manuscript writing with important intellectual content and approved the final version.</p><p>The project was supported by the Dam Foundation (Project ID: 2021/FO347301) through the Norwegian Health Association. YQS was supported by a Research grant from The Liaison Committee for Education, Research and Innovation in Central Norway (project ID 2018/42794).</p><p>There are no competing interests provided for any authors.</p><p>The sponsors had no role in study design, data collection, analysis, decision to publish, or manuscript preparation.</p><p>The study was approved by the Norwegian Regional Committees for Medical and Health Research Ethics (no. 31812). All HUNT participants have signed informed consent for participation and the use of data in research.</p>","PeriodicalId":17240,"journal":{"name":"Journal of the American Geriatrics Society","volume":"72 11","pages":"3590-3593"},"PeriodicalIF":4.5000,"publicationDate":"2024-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.19103","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Geriatrics Society","FirstCategoryId":"3","ListUrlMain":"https://agsjournals.onlinelibrary.wiley.com/doi/10.1111/jgs.19103","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Poor oral health and neurocognitive disorders (NCDs) are both important public health challenges in the general older population.1, 2 Older adults with NCDs may have poorer oral health due to decline in self-care, medication side effects, and lower dietary quality.3 Yet, the association between cognitive function and oral health is unclear.4 Wu et al. advocated a standardized assessment of oral health and cognitive states to better evaluate their potential associations.4
The aim of this cross-sectional study was to explore the relationship between cognitive function and oral health, both thoroughly assessed by clinical experts, in a home-dwelling Norwegian older adult population.
Our study population, derived from the Trøndelag Health Study Survey 4 (HUNT4), included 633 participants aged 70 years or older who attended both the HUNT4 Oral Health Study and HUNT4 70+.5-7
Clinical experts assessed the cognitive function of HUNT4 70+ participants after a comprehensive clinical evaluation, following the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria.7 In the current study, mild cognitive impairment (MCI) and dementia were diagnosed and collectively categorized as NCDs.
Participants in the HUNT4 Oral Health Study underwent clinical and radiographic examinations conducted by trained and calibrated dentists. Decayed, missing, and filled teeth (DMFT) were calculated using the clinical and radiographic caries registration of dental status.5 Decayed teeth were caries lesions confined in dentine (grades 3–5), secondary caries in dentine, and root caries with cavitation. Severe periodontitis was defined as periodontal Stage 3 or 4 based on radiographic bone loss and periodontal stage assessments.6
The relationships between cognitive function and the number of decayed teeth, DMFT or natural teeth were assessed using negative binomial regression models, computing ratios of means (RMs) with 95% confidence intervals (CIs). The relationship between cognitive function and the prevalence of severe periodontitis was estimated using Poisson regression with robust error variance, providing prevalence ratios (PRs) with 95% CIs. Covariates such as age, sex, education, marital status, body mass index (BMI), smoking status, and alcohol consumption were considered potential confounders based on the literature.4, 8, 9 All statistical analyses were performed with STATA/MP 18.
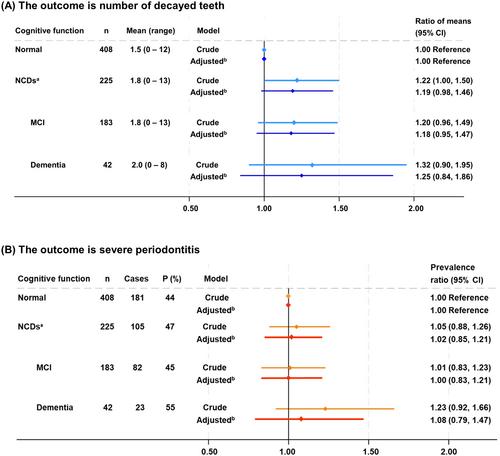
Table 1 describes the baseline characteristics of the study population overall and by cognitive function (normal and NCDs). As shown in Figure 1A, the mean number of decayed teeth was higher for participants with NCDs compared to those with normal cognitive function (1.8 vs. 1.5). NCDs were associated with a 19% increase in the mean number of decayed teeth in the adjusted model (RM 1.19, 95% CI 0.98–1.46), although it was not statistically significant (p-value = 0.09). It appears that a dose–response association was demonstrated (p-value for trend = 0.09): participants with MCI had an 18% increase (RM 1.18, 95% CI 0.95–1.47) in the mean number of decayed teeth, while those with dementia had a 25% increase (RM 1.25, 95% CI 0.84–1.86). There was no association between NCDs and the number of DMFT (Supplementary Table S1). Participants with dementia had a 9% decrease in the mean number of natural teeth compared to those with normal cognitive function (RM 0.91, 95% CI 0.84–0.99, Supplementary Table S2). The prevalence of severe periodontitis was similar among participants with NCDs compared to those with normal cognitive function (Figure 1B: PR 1.02, 95% CI 0.85–1.21).
Few studies have explored the relationships between cognitive function and clinically measured oral health components. The available measures were often limited to self-rated oral health, questionnaires, or non-dental screening tool.4, 8, 10 Our findings support the previous studies that reported an association between cognitive function and self-reported oral health.8, 10 Our study, along with previous research,10 suggests that poor cognitive function may lead to neglected self-care, resulting in poorer oral hygiene and oral health in older people.
The current study is one of the first to investigate potential associations between cognitive function and detailed oral health components, both clinically evaluated. NCDs were diagnosed by clinical experts, and oral health evaluation was thoroughly conducted by trained specialists in dentistry, which makes this study unique.5-7 However, the sample size was small, leading to relatively imprecise estimates with wider 95% CIs.
In conclusion, our results suggested that older adults with NCDs had a higher number of dental caries than those with normal cognitive function, and participants with dementia had fewer natural teeth. This highlights the need to improve the oral health care of home-dwelling older adults with NCDs.
MD wrote the initial draft of the manuscript. XMM and YQS performed the literature search and contributed to the study design. GS, HKS, and YQS were responsible for data collection. MD, EOA, and YQS conducted statistical analyses and interpreted results. MD, EOA, RSE, GS, HKS, XMM, YC, and YQS participated in the data interpretation and the manuscript writing with important intellectual content and approved the final version.
The project was supported by the Dam Foundation (Project ID: 2021/FO347301) through the Norwegian Health Association. YQS was supported by a Research grant from The Liaison Committee for Education, Research and Innovation in Central Norway (project ID 2018/42794).
There are no competing interests provided for any authors.
The sponsors had no role in study design, data collection, analysis, decision to publish, or manuscript preparation.
The study was approved by the Norwegian Regional Committees for Medical and Health Research Ethics (no. 31812). All HUNT participants have signed informed consent for participation and the use of data in research.
期刊介绍:
Journal of the American Geriatrics Society (JAGS) is the go-to journal for clinical aging research. We provide a diverse, interprofessional community of healthcare professionals with the latest insights on geriatrics education, clinical practice, and public policy—all supporting the high-quality, person-centered care essential to our well-being as we age. Since the publication of our first edition in 1953, JAGS has remained one of the oldest and most impactful journals dedicated exclusively to gerontology and geriatrics.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
