{"title":"Parkinson-like neurotoxicity in female patients treated with idecabtagene-vicleucel","authors":"Audrey Couturier, Martine Escoffre, Frédérique Leh, Anne-Sophie Villoteau, Xavier Palard, Florence Le Jeune, Olivier Decaux, Thierry Lamy, Roch Houot","doi":"10.1002/hem3.131","DOIUrl":null,"url":null,"abstract":"<p>Idecabtagene vicleucel (ide-cel) and ciltacabtagene autoleucel (cilta-cel) are two BCMA-directed CAR T-cells approved for the treatment of relapsed or refractory multiple myeloma. Similar to CD19-directed CAR T-cells, acute adverse events may occur after BCMA-directed CAR T-cells, including cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS). However, a new type of neurotoxicity has been recently reported in patients treated with BCMA-directed CAR T-cells, the so-called movement and neurocognitive toxicity (MNT). Common features include late onset of Parkinson-like symptoms such as tremor, bradykinesia, and neurocognitive disorder. Only 10 cases of MNT occurring after BCMA-directed CAR T-cells have been reported so far (Table 1). The symptoms appeared with a median time of 36 days (range, 14–914 days). Interestingly, all cases occurred in male patients and after cilta-cel except for one patient who had been treated with ide-cel.<span><sup>4</sup></span> MNT has been associated with high expansion and persistence of circulating CAR T-cells, cerebrospinal fluid infiltration by CAR T-cells, and no clear response to levodopa. Autopsy report from a patient who died shortly after presenting with MNT showed a T-cell infiltrate in the periventricular region of the basal ganglia as well as BCMA expression in the basal ganglia, suggesting an on-target off-tumor toxicity.<span><sup>1</sup></span> BCMA expression was also found on basal ganglia cells of healthy subjects.<span><sup>1</sup></span> Potential risk factors of MNT include high tumor burden at baseline before the start of lymphodepletion, grade ≥2 CRS, occurrence of ICANS, high CAR T-cell expansion, and prolonged persistence.<span><sup>1</sup></span> Management of this new and rare toxicity remains poorly defined. Corticosteroids, systemic chemotherapy, anakinra, intrathecal injections of cytarabine and steroids, IV Ig, and plasmaspharesis have been tested without clear benefit. Most patients experience mild or no improvement of their symptoms. In some patients, symptoms worsen and may lead to death.</p><p>Here, we report the case of two female patients who developed parkinsonism after ide-cel infusion.</p><p>Patient 1 is a 74-year-old woman who had been diagnosed with monoclonal gammopathy of unknown significance in 2003, which progressed to multiple myeloma in 2009. Before undergoing CAR T-cell therapy, she had received 11 prior lines of therapy including chemotherapy, IMIDs, proteasome inhibitors, daratumumab, and lastly talquetamab, a CD3/GPRC5D bispecific antibody. She was offered CAR T-cell therapy after developing lytic bone lesions while being treated with talquetamab. She received bridging therapy with Selinexor, which allowed partial metabolic response. After ide-cel infusion, she developed grade 1 CRS on Day 2 and no ICANS. She did not require treatment with tocilizumab nor dexamethasone. She was discharged on Day 10 postinfusion.</p><p>Immunofixation was negative 1 and 3 months after infusion (monoclonal spike was 3.7 g/L at baseline). [18F] FDG PET/CT evaluation after ide-cel infusion showed a partial response at 1 month and a complete response at 3 months.</p><p>At Day 36 after CAR T-cell infusion, the patient developed a discrete tremor along with mild psychomotor retardation. Cognitive and motor impairment worsened requiring hospitalization on Day 49 post CAR T-cell infusion. Clinically, she presented with Parkinson-like symptoms including asymmetric tremor, hypomimia, and rigidity. The symptoms worsened after a few days with severe rigidity, akinesia, and postural instability.</p><p>CAR T-cell monitoring showed high expansion and persistence of CAR T-cells with 92 CAR T-cells/µL at Day 7 and 374/µL at Day 35, by flow cytometry (Figure 1A). Similar to what has been previously reported, immunophenotyping of CD4 and CD8 CAR T-cells at Day 35 revealed that most CAR T-cells were EM-like (CD45RA−CCR7−), with a small proportion of EMRA-like CAR T-cells (CD45RA+CCR7−).<span><sup>6</sup></span> Brain MRI showed right-predominant bipallidal signal abnormalities of small extent, evolving in diffusion restriction with FLAIR hypersignal. Similar to other cases previously reported, <sup>123</sup>I-FP-CIT SPECT/CT scan was normal, suggesting integrity of the presynaptic dopaminergic transporters. [18F]FDG PET/CT showed decreased [18F]FDG activity in both striata (Figure 1B,C). CSF examination showed hyperproteinorrachia (0.83 g/L), normoglycorachia (4.62 mmol/L) with 23/mm<sup>3</sup> red blood cells (RBC) and 7/mm<sup>3</sup> leukocytes. By flow cytometry, 94% of lymphocytes were CAR T-cells.</p><p>On Day 56, while her neurologic condition continued to worsen, the patient was started on dopamine agonists and received systemic chemotherapy with fludarabine 30 mg/m²/day for 3 days as well as two intrathecal injections of methotrexate, aracytine, and methylprednisolone. Upon treatment, the patient showed rapid clinical improvement and was able to recover walking ability and sufficient autonomy to be discharged from the hospital on Day 88. CSF examination on Day 14 from the first intrathecal chemotherapy and Day 8 of IV Fludarabine showed complete clearance of CAR T-cells. Blood analysis at day 60 showed almost complete clearance of circulating CAR T-cells, down to 2 cells/µL (Figure 1A).</p><p>L-dopa test being negative, levodopa/carbidopa was progressively discontinued. The symptoms did not worsen after withdrawal of carbidopa/levodopa. Despite significant improvement, the patient did not fully recover and was still experiencing attitude and rest tremor of the four limbs with left-side predominance, severe rigidity, and bradykinesia as well as persisting apathy and dysexecutive symptomatology 3 months after fludarabine treatment. Follow-up brain MRI at day 118 revealed a marked reduction in diffusion hypersignal and T2 bi-pallidal signal anomalies predominantly on the right, although to a less marked extent (Figure 1D).</p><p>Patient 2 is a 73-year-old woman with penta-refractory multiple myeloma, first diagnosed in 2019. Following ide-cel treatment, she developed self-resolving grade 1 CRS and no ICANS, allowing discharge from the hospital on Day 12 after CAR T-cell infusion. The peak of CAR T-cell expansion was 261/µL at Day 10. At 1 month evaluation, [18F]FDG PET/CT showed a complete metabolic response while serum protein electrophoresis showed very good partial response with a monoclonal spike down to 4.8 g/L, against 44 g/L at baseline. Clinical assessment revealed the onset of Parkinson-like symptoms, including hypomimia, resting tremor, hypokinesia, and walking impairment. Neurologic evaluation found neurocognitive debilitation with severe apathy, and mnesic as well as executive difficulties. Lumbar puncture revealed lymphocytic meningitis, with 32% of lymphocytes being CAR T-cells as assessed by flow cytometry.</p><p>Brain MRI was unchanged compared to baseline, notably, there was no lesion of the basal ganglia. <sup>123</sup>I-FP-CIT SPECT/CT scan was normal. No significative improvement was observed after initiation of dopatherapy. The patient received a systemic chemotherapy with fludarabine 30 mg/m²/day for 3 days (from Day 42 to Day 44), and one intrathecal injection of methotrexate, aracytine, and methylprednisolone. This treatment induced a rapid and profound depletion of circulating CAR T-cells with less than 1 CAR T-cell/µL detectable at Day 75 of infusion. We observed a clinical, although partial, improvement with reduction of rigidity, hypokinesia, and tremor.</p><p>Despite successful depletion of CAR T-cells, none of the two patients experienced disease relapse/progression at last follow-up. Patient 1 remained in complete metabolic response at M6 with a negative immunofixation at M9. In patient 2, the monoclonal spike remained stable at 3.4 g/L at M3 versus 4.8 g/L before Fludarabine treatment.</p><p>These two cases have previously unreported features. First, to the best of our knowledge, these are the first reported cases of CAR T-cell induced-MNT occurring in female patients. Second, these are the second and third cases of MNT reported after ide-cel. Third, we were able to show for the first time abnormalities of the basal ganglia on brain MRI (patient 1), further supporting the pathophysiological mechanism associated with CAR T-cell-induced NRM neurotoxicity, explaining the lack of dopaminergic denervation and resistance to levodopa. Finally, we show for the first time that systemic fludarabine may be an effective treatment of MNT. Because MNT is thought to be due to the destruction of the basal ganglia by BCMA-directed CAR T-cells, we hypothesized that rapid depletion of CAR T-cells from the brain and CSF may be key to avoid irreversible neurologic damages. We chose to use fludarabine because it is a potent lymphodepleting chemotherapy which crosses the blood brain barrier.<span><sup>7</sup></span> The rapid clearance of CAR T-cells from the CSF along with the clinical improvement supports this strategy.</p><p>Movement and neurocognitive toxicity is a rare but potentially severe adverse event occurring in patients treated with BCMA-directed CAR T-cells. This toxicity has mostly been described in male patients and after cilta-cel treatment, but may occur in female patients and after ide-cel, as reported here. However, the exact sex ratio and the proportion of cilta-cel vs ide-cel in MNT patients remain unknown because cases are likely to be underreported and there is no exhaustive data to determine the percentage of MNT among all treated patients (based on sex and treatment characteristics). Therefore, the diagnosis of MNT should not be excluded/influenced based on sex nor CAR T-cell product. Furthermore, current understanding of the pathophysiology suggests direct destruction of the basal ganglia by BCMA-directed CAR T-cells. This supports the need for rapid eradication of CAR T-cells from the brain which may be achieved with systemic lymphodepleting chemotherapy, such as cyclophosphamide or fludarabine. Physicians should be aware of this rare toxicity to allow early recognition and rapid intervention in order to limit the risk of irreversible neurologic damages.</p><p>Roch Houot and Audrey Couturier conceived and wrote the original article. Xavier Palard, Florence Lejeune, Frédérique Leh, Anne-Sophie Villoteau, Martine Escoffre, Oliver Decaux and Thierry Lamy reviewed and edited the article. Xavier Palard, Florence Lejeune, and Anne-Sophie Villoteau helped with research and investigation for the article.</p><p>Roch Houot received honoraria from Kite/Gilead, Novartis, Incyte, Janssen, MSD, Takeda, and Roche; and consultancy at Kite/Gilead, 63 Novartis, Bristol-Myers Squibb/Celgene, ADC Therapeutics, Incyte, Miltenyi. Olivier Decaux received honoraria from Janssen, Celgene/BMS, Amgen, Takeda, GSK, Sanofi, Abbvie, Roche, The Binding Site, Sebia, Menarini-Stemline, and Pfizer. The remaining authors declare no competing financial interests.</p><p>This research received no funding.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 7","pages":""},"PeriodicalIF":14.6000,"publicationDate":"2024-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11270580/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.131","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Idecabtagene vicleucel (ide-cel) and ciltacabtagene autoleucel (cilta-cel) are two BCMA-directed CAR T-cells approved for the treatment of relapsed or refractory multiple myeloma. Similar to CD19-directed CAR T-cells, acute adverse events may occur after BCMA-directed CAR T-cells, including cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS). However, a new type of neurotoxicity has been recently reported in patients treated with BCMA-directed CAR T-cells, the so-called movement and neurocognitive toxicity (MNT). Common features include late onset of Parkinson-like symptoms such as tremor, bradykinesia, and neurocognitive disorder. Only 10 cases of MNT occurring after BCMA-directed CAR T-cells have been reported so far (Table 1). The symptoms appeared with a median time of 36 days (range, 14–914 days). Interestingly, all cases occurred in male patients and after cilta-cel except for one patient who had been treated with ide-cel.4 MNT has been associated with high expansion and persistence of circulating CAR T-cells, cerebrospinal fluid infiltration by CAR T-cells, and no clear response to levodopa. Autopsy report from a patient who died shortly after presenting with MNT showed a T-cell infiltrate in the periventricular region of the basal ganglia as well as BCMA expression in the basal ganglia, suggesting an on-target off-tumor toxicity.1 BCMA expression was also found on basal ganglia cells of healthy subjects.1 Potential risk factors of MNT include high tumor burden at baseline before the start of lymphodepletion, grade ≥2 CRS, occurrence of ICANS, high CAR T-cell expansion, and prolonged persistence.1 Management of this new and rare toxicity remains poorly defined. Corticosteroids, systemic chemotherapy, anakinra, intrathecal injections of cytarabine and steroids, IV Ig, and plasmaspharesis have been tested without clear benefit. Most patients experience mild or no improvement of their symptoms. In some patients, symptoms worsen and may lead to death.
Here, we report the case of two female patients who developed parkinsonism after ide-cel infusion.
Patient 1 is a 74-year-old woman who had been diagnosed with monoclonal gammopathy of unknown significance in 2003, which progressed to multiple myeloma in 2009. Before undergoing CAR T-cell therapy, she had received 11 prior lines of therapy including chemotherapy, IMIDs, proteasome inhibitors, daratumumab, and lastly talquetamab, a CD3/GPRC5D bispecific antibody. She was offered CAR T-cell therapy after developing lytic bone lesions while being treated with talquetamab. She received bridging therapy with Selinexor, which allowed partial metabolic response. After ide-cel infusion, she developed grade 1 CRS on Day 2 and no ICANS. She did not require treatment with tocilizumab nor dexamethasone. She was discharged on Day 10 postinfusion.
Immunofixation was negative 1 and 3 months after infusion (monoclonal spike was 3.7 g/L at baseline). [18F] FDG PET/CT evaluation after ide-cel infusion showed a partial response at 1 month and a complete response at 3 months.
At Day 36 after CAR T-cell infusion, the patient developed a discrete tremor along with mild psychomotor retardation. Cognitive and motor impairment worsened requiring hospitalization on Day 49 post CAR T-cell infusion. Clinically, she presented with Parkinson-like symptoms including asymmetric tremor, hypomimia, and rigidity. The symptoms worsened after a few days with severe rigidity, akinesia, and postural instability.
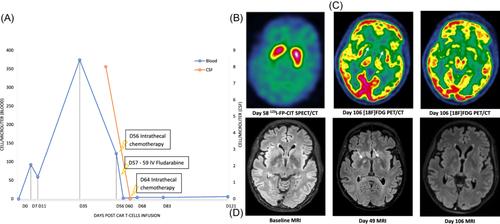
CAR T-cell monitoring showed high expansion and persistence of CAR T-cells with 92 CAR T-cells/µL at Day 7 and 374/µL at Day 35, by flow cytometry (Figure 1A). Similar to what has been previously reported, immunophenotyping of CD4 and CD8 CAR T-cells at Day 35 revealed that most CAR T-cells were EM-like (CD45RA−CCR7−), with a small proportion of EMRA-like CAR T-cells (CD45RA+CCR7−).6 Brain MRI showed right-predominant bipallidal signal abnormalities of small extent, evolving in diffusion restriction with FLAIR hypersignal. Similar to other cases previously reported, 123I-FP-CIT SPECT/CT scan was normal, suggesting integrity of the presynaptic dopaminergic transporters. [18F]FDG PET/CT showed decreased [18F]FDG activity in both striata (Figure 1B,C). CSF examination showed hyperproteinorrachia (0.83 g/L), normoglycorachia (4.62 mmol/L) with 23/mm3 red blood cells (RBC) and 7/mm3 leukocytes. By flow cytometry, 94% of lymphocytes were CAR T-cells.
On Day 56, while her neurologic condition continued to worsen, the patient was started on dopamine agonists and received systemic chemotherapy with fludarabine 30 mg/m²/day for 3 days as well as two intrathecal injections of methotrexate, aracytine, and methylprednisolone. Upon treatment, the patient showed rapid clinical improvement and was able to recover walking ability and sufficient autonomy to be discharged from the hospital on Day 88. CSF examination on Day 14 from the first intrathecal chemotherapy and Day 8 of IV Fludarabine showed complete clearance of CAR T-cells. Blood analysis at day 60 showed almost complete clearance of circulating CAR T-cells, down to 2 cells/µL (Figure 1A).
L-dopa test being negative, levodopa/carbidopa was progressively discontinued. The symptoms did not worsen after withdrawal of carbidopa/levodopa. Despite significant improvement, the patient did not fully recover and was still experiencing attitude and rest tremor of the four limbs with left-side predominance, severe rigidity, and bradykinesia as well as persisting apathy and dysexecutive symptomatology 3 months after fludarabine treatment. Follow-up brain MRI at day 118 revealed a marked reduction in diffusion hypersignal and T2 bi-pallidal signal anomalies predominantly on the right, although to a less marked extent (Figure 1D).
Patient 2 is a 73-year-old woman with penta-refractory multiple myeloma, first diagnosed in 2019. Following ide-cel treatment, she developed self-resolving grade 1 CRS and no ICANS, allowing discharge from the hospital on Day 12 after CAR T-cell infusion. The peak of CAR T-cell expansion was 261/µL at Day 10. At 1 month evaluation, [18F]FDG PET/CT showed a complete metabolic response while serum protein electrophoresis showed very good partial response with a monoclonal spike down to 4.8 g/L, against 44 g/L at baseline. Clinical assessment revealed the onset of Parkinson-like symptoms, including hypomimia, resting tremor, hypokinesia, and walking impairment. Neurologic evaluation found neurocognitive debilitation with severe apathy, and mnesic as well as executive difficulties. Lumbar puncture revealed lymphocytic meningitis, with 32% of lymphocytes being CAR T-cells as assessed by flow cytometry.
Brain MRI was unchanged compared to baseline, notably, there was no lesion of the basal ganglia. 123I-FP-CIT SPECT/CT scan was normal. No significative improvement was observed after initiation of dopatherapy. The patient received a systemic chemotherapy with fludarabine 30 mg/m²/day for 3 days (from Day 42 to Day 44), and one intrathecal injection of methotrexate, aracytine, and methylprednisolone. This treatment induced a rapid and profound depletion of circulating CAR T-cells with less than 1 CAR T-cell/µL detectable at Day 75 of infusion. We observed a clinical, although partial, improvement with reduction of rigidity, hypokinesia, and tremor.
Despite successful depletion of CAR T-cells, none of the two patients experienced disease relapse/progression at last follow-up. Patient 1 remained in complete metabolic response at M6 with a negative immunofixation at M9. In patient 2, the monoclonal spike remained stable at 3.4 g/L at M3 versus 4.8 g/L before Fludarabine treatment.
These two cases have previously unreported features. First, to the best of our knowledge, these are the first reported cases of CAR T-cell induced-MNT occurring in female patients. Second, these are the second and third cases of MNT reported after ide-cel. Third, we were able to show for the first time abnormalities of the basal ganglia on brain MRI (patient 1), further supporting the pathophysiological mechanism associated with CAR T-cell-induced NRM neurotoxicity, explaining the lack of dopaminergic denervation and resistance to levodopa. Finally, we show for the first time that systemic fludarabine may be an effective treatment of MNT. Because MNT is thought to be due to the destruction of the basal ganglia by BCMA-directed CAR T-cells, we hypothesized that rapid depletion of CAR T-cells from the brain and CSF may be key to avoid irreversible neurologic damages. We chose to use fludarabine because it is a potent lymphodepleting chemotherapy which crosses the blood brain barrier.7 The rapid clearance of CAR T-cells from the CSF along with the clinical improvement supports this strategy.
Movement and neurocognitive toxicity is a rare but potentially severe adverse event occurring in patients treated with BCMA-directed CAR T-cells. This toxicity has mostly been described in male patients and after cilta-cel treatment, but may occur in female patients and after ide-cel, as reported here. However, the exact sex ratio and the proportion of cilta-cel vs ide-cel in MNT patients remain unknown because cases are likely to be underreported and there is no exhaustive data to determine the percentage of MNT among all treated patients (based on sex and treatment characteristics). Therefore, the diagnosis of MNT should not be excluded/influenced based on sex nor CAR T-cell product. Furthermore, current understanding of the pathophysiology suggests direct destruction of the basal ganglia by BCMA-directed CAR T-cells. This supports the need for rapid eradication of CAR T-cells from the brain which may be achieved with systemic lymphodepleting chemotherapy, such as cyclophosphamide or fludarabine. Physicians should be aware of this rare toxicity to allow early recognition and rapid intervention in order to limit the risk of irreversible neurologic damages.
Roch Houot and Audrey Couturier conceived and wrote the original article. Xavier Palard, Florence Lejeune, Frédérique Leh, Anne-Sophie Villoteau, Martine Escoffre, Oliver Decaux and Thierry Lamy reviewed and edited the article. Xavier Palard, Florence Lejeune, and Anne-Sophie Villoteau helped with research and investigation for the article.
Roch Houot received honoraria from Kite/Gilead, Novartis, Incyte, Janssen, MSD, Takeda, and Roche; and consultancy at Kite/Gilead, 63 Novartis, Bristol-Myers Squibb/Celgene, ADC Therapeutics, Incyte, Miltenyi. Olivier Decaux received honoraria from Janssen, Celgene/BMS, Amgen, Takeda, GSK, Sanofi, Abbvie, Roche, The Binding Site, Sebia, Menarini-Stemline, and Pfizer. The remaining authors declare no competing financial interests.
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
