Michael J Lydeamore, Tjibbe Donker, David Wu, Claire Gorrie, Annabelle Turner, Marion Easton, Daneeta Hennessy, Nicholas Geard, Benjamin P Howden, Ben S Cooper, Andrew Wilson, Anton Y Peleg, Andrew J Stewardson
{"title":"Carbapenemase-producing enterobacterales colonisation status does not lead to more frequent admissions: a linked patient study.","authors":"Michael J Lydeamore, Tjibbe Donker, David Wu, Claire Gorrie, Annabelle Turner, Marion Easton, Daneeta Hennessy, Nicholas Geard, Benjamin P Howden, Ben S Cooper, Andrew Wilson, Anton Y Peleg, Andrew J Stewardson","doi":"10.1186/s13756-024-01437-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hospitals in any given region can be considered as part of a network, where facilities are connected to one another - and hospital pathogens potentially spread - through the movement of patients between them. We sought to describe the hospital admission patterns of patients known to be colonised with carbapenemase-producing Enterobacterales (CPE), and compare them with CPE-negative patient cohorts, matched on comorbidity information.</p><p><strong>Methods: </strong>We performed a linkage study in Victoria, Australia, including datasets with notifiable diseases (CPE notifications) and hospital admissions (admission dates and diagnostic codes) for the period 2011 to 2020. Where the CPE notification date occurred during a hospital admission for the same patient, we identified this as the 'index admission'. We determined the number of distinct health services each patient was admitted to, and time to first admission to a different health service. We compared CPE-positive patients with four cohorts of CPE-negative patients, sampled based on different matching criteria.</p><p><strong>Results: </strong>Of 528 unique patients who had CPE detected during a hospital admission, 222 (42%) were subsequently admitted to a different health service during the study period. Among these patients, CPE diagnosis tended to occur during admission to a metropolitan public hospital (86%, 190/222), whereas there was a greater number of metropolitan private (23%, 52/222) and rural public (18%, 39/222) hospitals for the subsequent admission. Median time to next admission was 4 days (IQR, 0-75 days). Admission patterns for CPE-positive patients was similar to the cohort of CPE-negative patients matched on index admission, time period, and age-adjusted Charlson comorbidity index.</p><p><strong>Conclusions: </strong>Movement of CPE-positive patients between health services is not a rare event. While the most common movement is from one public metropolitan health service to another, there is also a trend for movement from metropolitan public hospitals into private and rural hospitals. After accounting for clinical comorbidities, CPE colonisation status does not appear to impact on hospital admission frequency or timing. These findings support the potential utility of a centralised notification and outbreak management system for CPE positive patients.</p>","PeriodicalId":7950,"journal":{"name":"Antimicrobial Resistance and Infection Control","volume":"13 1","pages":"82"},"PeriodicalIF":4.4000,"publicationDate":"2024-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11287836/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Antimicrobial Resistance and Infection Control","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13756-024-01437-x","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Hospitals in any given region can be considered as part of a network, where facilities are connected to one another - and hospital pathogens potentially spread - through the movement of patients between them. We sought to describe the hospital admission patterns of patients known to be colonised with carbapenemase-producing Enterobacterales (CPE), and compare them with CPE-negative patient cohorts, matched on comorbidity information.
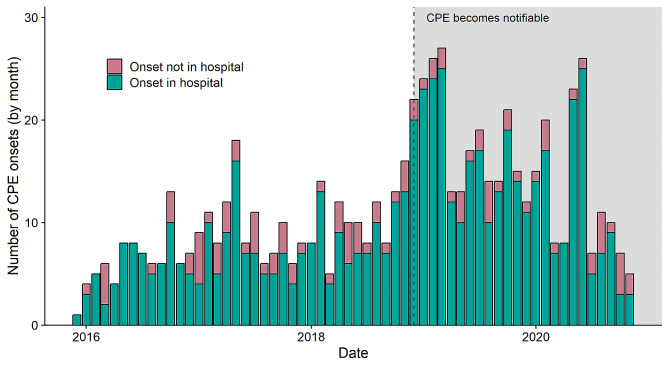
Methods: We performed a linkage study in Victoria, Australia, including datasets with notifiable diseases (CPE notifications) and hospital admissions (admission dates and diagnostic codes) for the period 2011 to 2020. Where the CPE notification date occurred during a hospital admission for the same patient, we identified this as the 'index admission'. We determined the number of distinct health services each patient was admitted to, and time to first admission to a different health service. We compared CPE-positive patients with four cohorts of CPE-negative patients, sampled based on different matching criteria.
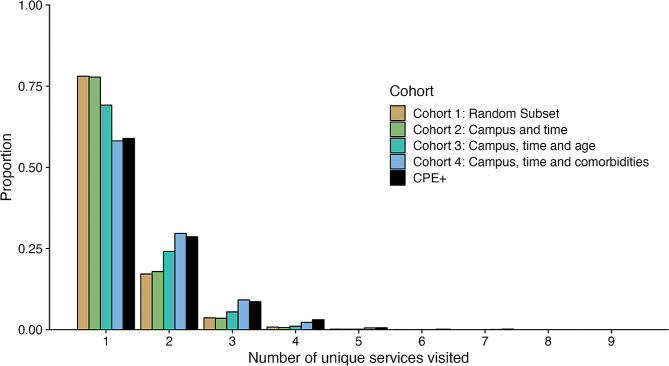
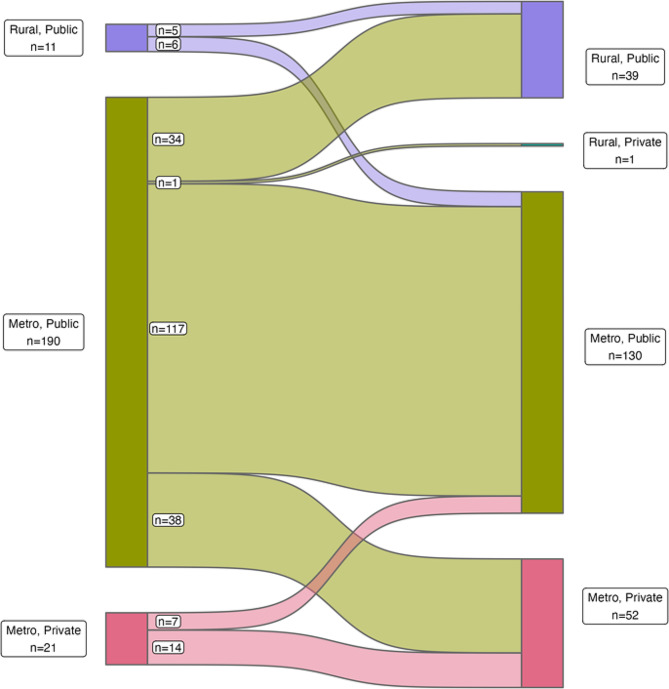
Results: Of 528 unique patients who had CPE detected during a hospital admission, 222 (42%) were subsequently admitted to a different health service during the study period. Among these patients, CPE diagnosis tended to occur during admission to a metropolitan public hospital (86%, 190/222), whereas there was a greater number of metropolitan private (23%, 52/222) and rural public (18%, 39/222) hospitals for the subsequent admission. Median time to next admission was 4 days (IQR, 0-75 days). Admission patterns for CPE-positive patients was similar to the cohort of CPE-negative patients matched on index admission, time period, and age-adjusted Charlson comorbidity index.
Conclusions: Movement of CPE-positive patients between health services is not a rare event. While the most common movement is from one public metropolitan health service to another, there is also a trend for movement from metropolitan public hospitals into private and rural hospitals. After accounting for clinical comorbidities, CPE colonisation status does not appear to impact on hospital admission frequency or timing. These findings support the potential utility of a centralised notification and outbreak management system for CPE positive patients.
期刊介绍:
Antimicrobial Resistance and Infection Control is a global forum for all those working on the prevention, diagnostic and treatment of health-care associated infections and antimicrobial resistance development in all health-care settings. The journal covers a broad spectrum of preeminent practices and best available data to the top interventional and translational research, and innovative developments in the field of infection control.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
