Simon Schneekloth, Mogens Krøigaard, Johannes K. Boysen, Holger Mosbech, Birgitte B. Melchiors, Lene H. Garvey
{"title":"Oral Tolerance in Patients With Allergy to Patent Blue V—A 20-Year Single Centre Experience","authors":"Simon Schneekloth, Mogens Krøigaard, Johannes K. Boysen, Holger Mosbech, Birgitte B. Melchiors, Lene H. Garvey","doi":"10.1111/cea.14534","DOIUrl":null,"url":null,"abstract":"<p>Blue dyes are a common cause of perioperative hypersensitivity (POH) reactions, with studies reporting 1:300 patients having reactions ranging from localised urticaria to circulatory collapse [<span>1</span>].</p><p>Sentinel lymph node biopsy (SLNB) is the gold standard in early-stage breast cancer detection, using the combination of blue dye and isotope tracing with an identification rate of 98.8% [<span>2</span>]. The mode of sensitisation to patent blue V (PBV) is unknown as patients typically react on their first subcutaneous exposure. PBV is also used to colour products such as textiles, food and cosmetics, and exposure to PBV is almost inevitable in daily life. However, no information is available regarding potential risks of allergic reactions to PBV, through such exposure, after confirmed allergy to subcutaneous exposure. After a suspected POH reaction, it is important to refer patients for allergy investigation to identify the culprit drug and find a safe alternative [<span>3</span>].</p><p>The aims of this single-centre retrospective study were to identify patients investigated for suspected POH to PBV, characterise reactions, determine the proportion of patients with confirmed allergy to PBV and to evaluate the frequency of oral tolerance among patients with confirmed allergy to subcutaneously administered PBV.</p><p>Data were collected from the Danish Anaesthesia Allergy Centre (DAAC) database from 2004 to 2023 and included clinical history, symptoms from the POH reaction, results of skin tests, in-vitro tests and drug provocation in 843 patients.</p><p>In total, 843 patients had been investigated and 75 (8.9%) had been exposed to PBV prior to the suspected POH reaction and were included in the study. Included patients were predominantly women (<i>n</i> = 68, 91%, mean age: 56 years) with breast cancer. Of the 75 patients, 54 (72%) were diagnosed with PBV hypersensitivity. Symptoms occurred <30 min after injection in 30 cases (67%) and >30 min after injection in 15 cases (33%), unknown in 9 patients. Of the 21 patients testing negative to PBV, two tested positive to dicloxacillin and chlorhexidine, respectively. Of patients testing positive to PBV 28 (52%) suffered grade III reactions (modified Ring and Messmer classification [<span>3</span>]), meeting the criteria for anaphylaxis; 19 had grade I reactions, of which 6 had localised urticaria and 10 had generalised urticaria.</p><p>Diagnosis of allergy to PBV were made by skin prick test (SPT) in concentrations of 0.25, 2.5 and 25 mg/mL and intradermal test (IDT) in concentrations of 0.025 and 0.25 mg/mL. In total, 52 out of 54 patients with proven hypersensitivity to PBV underwent titrated sublingual and oral provocation up to 30 mg of PBV. This was tolerated by all patients. The protocol used for oral challenge with PBV is shown in Figure 1.</p><p>To our knowledge, this retrospective single-centre study presents the largest series of patients with PBV allergy so far and provides important information on clinical features and investigation results. It is also the first study to address oral tolerance to PBV in patients with confirmed allergy.</p><p>This has important implications for patients, who do not need to avoid exposure in their daily life. This is consistent with oral tolerance being described in patients with allergy to parenteral exposure to other substances such as carboxymethylcellulose [<span>3, 4</span>]. This suggests differences in activation of the immune system on oral/sublingual and subcutaneous exposure, respectively.</p><p>Through 20 years of data on POH reactions to PBV available in DAAC, there were no cases of cardiac arrest or permanent injury, but 52% had reactions meeting the criteria for anaphylaxis. Balancing the risk of possible adverse effects to blue dyes against the improving the diagnostic value has been debated in the literature, emphasising the relatively high risk of allergic reactions including anaphylaxis. Currently there is no consensus as some studies suggest adding PBV in SLNB is needed to increase the sensitivity of the procedure, others do not find increased sensitivity when adding PBV [<span>2, 5</span>].</p><p>A meta-analysis quantified the risk of anaphylaxis to various blue dyes, and it was noted that a volume <2.0 mL and intradermal injection reduced the risk of anaphylaxis. The use of PBV in patients with melanoma allows intradermal injections, while the dye is injected parenchymally and typically at a larger volume in patients with breast cancer. Melanoma patients have been shown to have a 19-fold reduced risk of blue dye induced anaphylaxis, when compared to patients with breast cancer [<span>6</span>]. Unfortunately, we were not able to evaluate whether dosage of PBV correlated to severity of allergic reactions as information about dosage was not available in the majority of cases.</p><p>Limitations of our study includes the retrospective method and potential selection bias either due to minor localised allergic reactions to PBV being overlooked or just concluded to be due to PBV without referring for allergy investigation at DAAC.</p><p>Future studies should address how patients are sensitised to PBV and why sensitisation does not lead to clinical reactions on oral exposure. In addition, studies should investigate potential risk factors for allergic reactions, such as administration route and injected volume, with an aim to reduce the incidence of these reactions.</p><p>In conclusion, PBV tested positive in 72% of patients who had a POH reaction during surgery, where PBV had been administered, and it caused both localised and severe reactions. Patients with proven hypersensitivity to patent blue V tolerate oral exposure and do not need to avoid patent blue V in foods, drinks and textiles.</p><p>Conception and design: L.H.G., M.K., H.M. Acquisition of data: B.B.M., L.H.G., M.K., H.M. Data analysis and interpretation of data: S.S., J.K.B., B.B.M., L.H.G. Drafting the manuscript: S.S., L.H.G. Critical revision for important intellectual content and final approval: S.S., J.K.B., B.B.M., L.H.G., M.K., H.M.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":10207,"journal":{"name":"Clinical and Experimental Allergy","volume":"54 10","pages":"763-765"},"PeriodicalIF":5.2000,"publicationDate":"2024-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cea.14534","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cea.14534","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Blue dyes are a common cause of perioperative hypersensitivity (POH) reactions, with studies reporting 1:300 patients having reactions ranging from localised urticaria to circulatory collapse [1].
Sentinel lymph node biopsy (SLNB) is the gold standard in early-stage breast cancer detection, using the combination of blue dye and isotope tracing with an identification rate of 98.8% [2]. The mode of sensitisation to patent blue V (PBV) is unknown as patients typically react on their first subcutaneous exposure. PBV is also used to colour products such as textiles, food and cosmetics, and exposure to PBV is almost inevitable in daily life. However, no information is available regarding potential risks of allergic reactions to PBV, through such exposure, after confirmed allergy to subcutaneous exposure. After a suspected POH reaction, it is important to refer patients for allergy investigation to identify the culprit drug and find a safe alternative [3].
The aims of this single-centre retrospective study were to identify patients investigated for suspected POH to PBV, characterise reactions, determine the proportion of patients with confirmed allergy to PBV and to evaluate the frequency of oral tolerance among patients with confirmed allergy to subcutaneously administered PBV.
Data were collected from the Danish Anaesthesia Allergy Centre (DAAC) database from 2004 to 2023 and included clinical history, symptoms from the POH reaction, results of skin tests, in-vitro tests and drug provocation in 843 patients.
In total, 843 patients had been investigated and 75 (8.9%) had been exposed to PBV prior to the suspected POH reaction and were included in the study. Included patients were predominantly women (n = 68, 91%, mean age: 56 years) with breast cancer. Of the 75 patients, 54 (72%) were diagnosed with PBV hypersensitivity. Symptoms occurred <30 min after injection in 30 cases (67%) and >30 min after injection in 15 cases (33%), unknown in 9 patients. Of the 21 patients testing negative to PBV, two tested positive to dicloxacillin and chlorhexidine, respectively. Of patients testing positive to PBV 28 (52%) suffered grade III reactions (modified Ring and Messmer classification [3]), meeting the criteria for anaphylaxis; 19 had grade I reactions, of which 6 had localised urticaria and 10 had generalised urticaria.
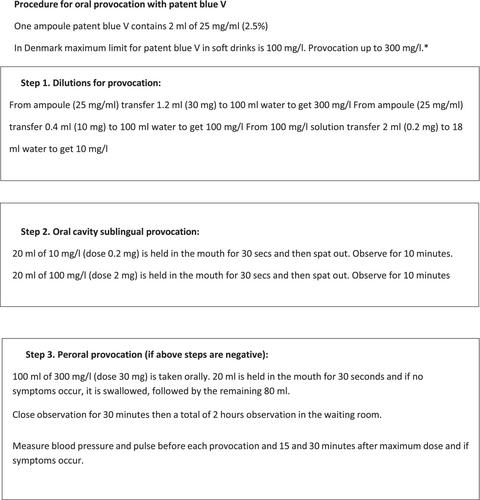
Diagnosis of allergy to PBV were made by skin prick test (SPT) in concentrations of 0.25, 2.5 and 25 mg/mL and intradermal test (IDT) in concentrations of 0.025 and 0.25 mg/mL. In total, 52 out of 54 patients with proven hypersensitivity to PBV underwent titrated sublingual and oral provocation up to 30 mg of PBV. This was tolerated by all patients. The protocol used for oral challenge with PBV is shown in Figure 1.
To our knowledge, this retrospective single-centre study presents the largest series of patients with PBV allergy so far and provides important information on clinical features and investigation results. It is also the first study to address oral tolerance to PBV in patients with confirmed allergy.
This has important implications for patients, who do not need to avoid exposure in their daily life. This is consistent with oral tolerance being described in patients with allergy to parenteral exposure to other substances such as carboxymethylcellulose [3, 4]. This suggests differences in activation of the immune system on oral/sublingual and subcutaneous exposure, respectively.
Through 20 years of data on POH reactions to PBV available in DAAC, there were no cases of cardiac arrest or permanent injury, but 52% had reactions meeting the criteria for anaphylaxis. Balancing the risk of possible adverse effects to blue dyes against the improving the diagnostic value has been debated in the literature, emphasising the relatively high risk of allergic reactions including anaphylaxis. Currently there is no consensus as some studies suggest adding PBV in SLNB is needed to increase the sensitivity of the procedure, others do not find increased sensitivity when adding PBV [2, 5].
A meta-analysis quantified the risk of anaphylaxis to various blue dyes, and it was noted that a volume <2.0 mL and intradermal injection reduced the risk of anaphylaxis. The use of PBV in patients with melanoma allows intradermal injections, while the dye is injected parenchymally and typically at a larger volume in patients with breast cancer. Melanoma patients have been shown to have a 19-fold reduced risk of blue dye induced anaphylaxis, when compared to patients with breast cancer [6]. Unfortunately, we were not able to evaluate whether dosage of PBV correlated to severity of allergic reactions as information about dosage was not available in the majority of cases.
Limitations of our study includes the retrospective method and potential selection bias either due to minor localised allergic reactions to PBV being overlooked or just concluded to be due to PBV without referring for allergy investigation at DAAC.
Future studies should address how patients are sensitised to PBV and why sensitisation does not lead to clinical reactions on oral exposure. In addition, studies should investigate potential risk factors for allergic reactions, such as administration route and injected volume, with an aim to reduce the incidence of these reactions.
In conclusion, PBV tested positive in 72% of patients who had a POH reaction during surgery, where PBV had been administered, and it caused both localised and severe reactions. Patients with proven hypersensitivity to patent blue V tolerate oral exposure and do not need to avoid patent blue V in foods, drinks and textiles.
Conception and design: L.H.G., M.K., H.M. Acquisition of data: B.B.M., L.H.G., M.K., H.M. Data analysis and interpretation of data: S.S., J.K.B., B.B.M., L.H.G. Drafting the manuscript: S.S., L.H.G. Critical revision for important intellectual content and final approval: S.S., J.K.B., B.B.M., L.H.G., M.K., H.M.
期刊介绍:
Clinical & Experimental Allergy strikes an excellent balance between clinical and scientific articles and carries regular reviews and editorials written by leading authorities in their field.
In response to the increasing number of quality submissions, since 1996 the journals size has increased by over 30%. Clinical & Experimental Allergy is essential reading for allergy practitioners and research scientists with an interest in allergic diseases and mechanisms. Truly international in appeal, Clinical & Experimental Allergy publishes clinical and experimental observations in disease in all fields of medicine in which allergic hypersensitivity plays a part.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
