Masato Fukae, Kyle Baron, Masaya Tachibana, John Mondick, Takako Shimizu
{"title":"Population pharmacokinetics of total and unbound valemetostat and platelet dynamics in healthy volunteers and patients with non-Hodgkin lymphoma","authors":"Masato Fukae, Kyle Baron, Masaya Tachibana, John Mondick, Takako Shimizu","doi":"10.1002/psp4.13201","DOIUrl":null,"url":null,"abstract":"<p>Valemetostat is an EZH2/1 inhibitor that has been approved in Japan for the treatment of patients with relapsed/refractory adult T-cell leukemia/lymphoma, based mainly on results from a single-arm phase II trial. It is currently under investigation worldwide for the treatment of other non-Hodgkin lymphomas (NHLs), including peripheral T-cell lymphoma, and for solid tumors. Semi-mechanistic population pharmacokinetic modeling of total and unbound valemetostat and an analysis of the platelet time course during treatment with valemetostat were conducted using data from five clinical trials (two in patients with NHL and three in healthy volunteers). Pharmacokinetic data, including 3162 total/1871 unbound valemetostat observations from 102 patients and 72 healthy volunteers, were described by a three-compartment model with sequential zero-/first-order absorption and saturable binding in the central compartment. Alpha-1-acid glycoprotein (AAG) was the most influential covariate for total valemetostat exposure, yet had little impact on unbound exposure, meaning no dose adjustment was warranted based on AAG levels. The longitudinal platelet data from 101 patients (2313 observations) were adequately described by a modified Friberg model with two proliferation compartments, which characterized unique spontaneous recovery of platelet counts without dose modifications. A model-based simulation quantitatively assessed the proposed dose-adjustment guidance in case of platelet count decreased by comparing the probability of treatment discontinuation due to platelet count decreased with or without the dose adjustment. In summary, the models described observed total and unbound valemetostat concentrations and a unique time course of platelets during treatment, which can justify the clinical dose and provide dose-adjustment guidance.</p>","PeriodicalId":10774,"journal":{"name":"CPT: Pharmacometrics & Systems Pharmacology","volume":"13 10","pages":"1641-1654"},"PeriodicalIF":3.0000,"publicationDate":"2024-07-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11494923/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CPT: Pharmacometrics & Systems Pharmacology","FirstCategoryId":"3","ListUrlMain":"https://ascpt.onlinelibrary.wiley.com/doi/10.1002/psp4.13201","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
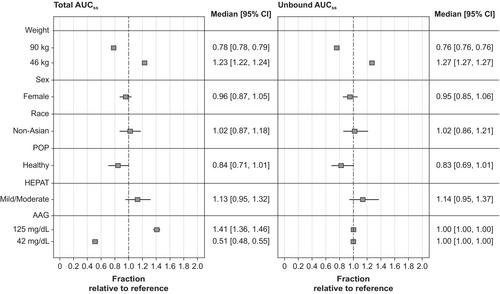
Valemetostat is an EZH2/1 inhibitor that has been approved in Japan for the treatment of patients with relapsed/refractory adult T-cell leukemia/lymphoma, based mainly on results from a single-arm phase II trial. It is currently under investigation worldwide for the treatment of other non-Hodgkin lymphomas (NHLs), including peripheral T-cell lymphoma, and for solid tumors. Semi-mechanistic population pharmacokinetic modeling of total and unbound valemetostat and an analysis of the platelet time course during treatment with valemetostat were conducted using data from five clinical trials (two in patients with NHL and three in healthy volunteers). Pharmacokinetic data, including 3162 total/1871 unbound valemetostat observations from 102 patients and 72 healthy volunteers, were described by a three-compartment model with sequential zero-/first-order absorption and saturable binding in the central compartment. Alpha-1-acid glycoprotein (AAG) was the most influential covariate for total valemetostat exposure, yet had little impact on unbound exposure, meaning no dose adjustment was warranted based on AAG levels. The longitudinal platelet data from 101 patients (2313 observations) were adequately described by a modified Friberg model with two proliferation compartments, which characterized unique spontaneous recovery of platelet counts without dose modifications. A model-based simulation quantitatively assessed the proposed dose-adjustment guidance in case of platelet count decreased by comparing the probability of treatment discontinuation due to platelet count decreased with or without the dose adjustment. In summary, the models described observed total and unbound valemetostat concentrations and a unique time course of platelets during treatment, which can justify the clinical dose and provide dose-adjustment guidance.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
