Assessing the Safety of Early Repatriation for Stable ST-Segment Elevation Myocardial Infarction Patients After Primary Percutaneous Coronary Intervention
Razi Khan MD, MSc , Shanjot Brar MD , Farshad Hosseini MD , Nazmul Karim MBBS, MPH, PhD , Natasha Kohli RN , Robert Yao MD , Albert Chan MD , Jahangir Charania MD , Roger Philipp MD , Minh Vo MD , Tycho Vuurmans MD, PhD
{"title":"Assessing the Safety of Early Repatriation for Stable ST-Segment Elevation Myocardial Infarction Patients After Primary Percutaneous Coronary Intervention","authors":"Razi Khan MD, MSc , Shanjot Brar MD , Farshad Hosseini MD , Nazmul Karim MBBS, MPH, PhD , Natasha Kohli RN , Robert Yao MD , Albert Chan MD , Jahangir Charania MD , Roger Philipp MD , Minh Vo MD , Tycho Vuurmans MD, PhD","doi":"10.1016/j.cjco.2024.07.010","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>Repatriation of ST-segment elevation myocardial infarction (STEMI) patients after primary percutaneous coronary intervention (PPCI) is common in regional health care programs. We examined the short- and long-term safety of early repatriation after PPCI in stable STEMI patients.</div></div><div><h3>Methods</h3><div>Consecutive stable STEMI patients undergoing PPCI between 2016 to 2018 in the Fraser Health Authority were included. Outcomes were compared between early and nonrepatriated cohorts. Co-primary outcomes were a composite of death, myocardial infarction, congestive heart failure, and stroke at 30 days and 1 year. Logistic regression analyses were performed to determine association between early repatriation and outcomes, and to assess impact of transfer to cardiologist- vs internist-based care centres.</div></div><div><h3>Results</h3><div>A total of 788 patients were included, with 62% being repatriated early. Primary composite and individual outcomes rates were similar between both cohorts. Early repatriation was not an independent predictor of 30-day (odds ratio [OR] 0.93, 95% confidence interval [CI] 0.50-1.72; <em>P</em> = 0.82) or 1-year (OR 1.05, 95% CI 0.67-1.65; <em>P</em> = 0.8) primary outcome, or of 30-day (OR 1.35, 95% CI 0.41-4.47, <em>P</em> = 0.63) or 1-year (OR 1.03, 95% CI 0.44-2.40; <em>P</em> = 0.95) mortality. Among early repatriated patients, transfer to cardiologist- vs internist-based care centres was not an independent factor for 30-day (OR 1.07, 95% CI 0.45-2.54; <em>P</em> = 0.87) or 1-year (OR 1.17, 95% 0.55-2.50, <em>P</em> = 0.69) primary outcome.</div></div><div><h3>Conclusions</h3><div>Early repatriation of stable STEMI patients after PPCI appears to be safe based on short- and long-term outcomes, and transfer to internist- vs cardiology-based centres did not affect outcomes. After PPCI, early repatriation allows for redistribution of stable STEMI patients to lower-acuity settings across regional hospitals.</div></div>","PeriodicalId":36924,"journal":{"name":"CJC Open","volume":"6 11","pages":"Pages 1289-1298"},"PeriodicalIF":2.5000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CJC Open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2589790X24003160","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/24 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Repatriation of ST-segment elevation myocardial infarction (STEMI) patients after primary percutaneous coronary intervention (PPCI) is common in regional health care programs. We examined the short- and long-term safety of early repatriation after PPCI in stable STEMI patients.
Methods
Consecutive stable STEMI patients undergoing PPCI between 2016 to 2018 in the Fraser Health Authority were included. Outcomes were compared between early and nonrepatriated cohorts. Co-primary outcomes were a composite of death, myocardial infarction, congestive heart failure, and stroke at 30 days and 1 year. Logistic regression analyses were performed to determine association between early repatriation and outcomes, and to assess impact of transfer to cardiologist- vs internist-based care centres.
Results
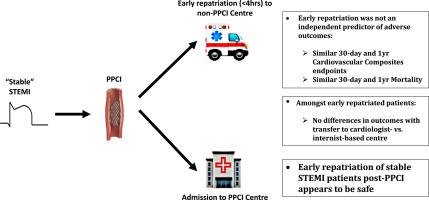
A total of 788 patients were included, with 62% being repatriated early. Primary composite and individual outcomes rates were similar between both cohorts. Early repatriation was not an independent predictor of 30-day (odds ratio [OR] 0.93, 95% confidence interval [CI] 0.50-1.72; P = 0.82) or 1-year (OR 1.05, 95% CI 0.67-1.65; P = 0.8) primary outcome, or of 30-day (OR 1.35, 95% CI 0.41-4.47, P = 0.63) or 1-year (OR 1.03, 95% CI 0.44-2.40; P = 0.95) mortality. Among early repatriated patients, transfer to cardiologist- vs internist-based care centres was not an independent factor for 30-day (OR 1.07, 95% CI 0.45-2.54; P = 0.87) or 1-year (OR 1.17, 95% 0.55-2.50, P = 0.69) primary outcome.
Conclusions
Early repatriation of stable STEMI patients after PPCI appears to be safe based on short- and long-term outcomes, and transfer to internist- vs cardiology-based centres did not affect outcomes. After PPCI, early repatriation allows for redistribution of stable STEMI patients to lower-acuity settings across regional hospitals.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
