{"title":"Real-world retrospective analysis of immune checkpoint inhibitor therapy for relapsed or refractory Hodgkin's lymphoma.","authors":"Tatsuo Oyake, Takahiro Maeta, Takenori Takahata, Yoshiko Tamai, Yoshihiro Kameoka, Naoto Takahashi, Yasuro Miyairi, Kazunori Murai, Kenji Shimosegawa, Kozue Yoshida, Kyoko Inokura, Noriko Fukuhara, Hideo Harigae, Ryo Sato, Kenichi Ishizawa, Katsushi Tajima, Souichi Saitou, Masahiko Fukatsu, Takayuki Ikezoe, Saburo Tsunoda, Masayuki Mita, Jinichi Mori, Shugo Kowata, Shigeki Ito","doi":"10.3960/jslrt.24021","DOIUrl":null,"url":null,"abstract":"<p><p>Immune checkpoint inhibitors (ICI) are promising therapeutic agents for relapsed or refractory classical Hodgkin's lymphoma (RRcHL). This retrospective study evaluated patients with RRcHL registered in the clinical research program Tohoku-Hematology-Forum-26, between 2016 and 2020, and treated with ICI in 14 centers in Northeast Japan. We analyzed the usage, efficacy, and safety of ICI therapy (ICIT). Among a total of 27 patients with RRcHL, 21 and nine were treated with nivolumab and/or pembrolizumab, respectively. The best response was complete response (CR), partial response (PR), stable disease (SD), and progressive disease in 11 (40.8%), seven (25.9%), eight (29.6%), and one (3.7%) patient, respectively. In all patients undergoing ICIT, the 2-year progression-free survival and 2-year overall survival (OS) were 48.6% and 87.4%, respectively. The 2-year OS for patients with CR, PR, and SD were 100%, 68.6%, and 87.5%, respectively. A total of 36 events of immune-related adverse events (irAEs) or immune-related like adverse events (irlAEs) were observed in 19 of the 27 patients (70.4%). Two thirds of these irAEs or irlAEs were grade 1-2 and controllable. During the observation period, ICIT was discontinued in 22 of 27 (81.4%) patients due to CR, inadequate response, irAE and patient circumstances in five (22.7%), seven (31.8%), eight (36.4%) and two patients (9.1%), respectively. Therapy-related mortality-associated irAE were observed in only one patient during ICIT. These results suggest that ICIT for RRcHL is effective and safe in real-world settings. The optimal timing of induction and duration of ICIT remains to be established.</p>","PeriodicalId":45936,"journal":{"name":"Journal of Clinical and Experimental Hematopathology","volume":" ","pages":"191-202"},"PeriodicalIF":1.4000,"publicationDate":"2024-09-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11528253/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Experimental Hematopathology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3960/jslrt.24021","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/31 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
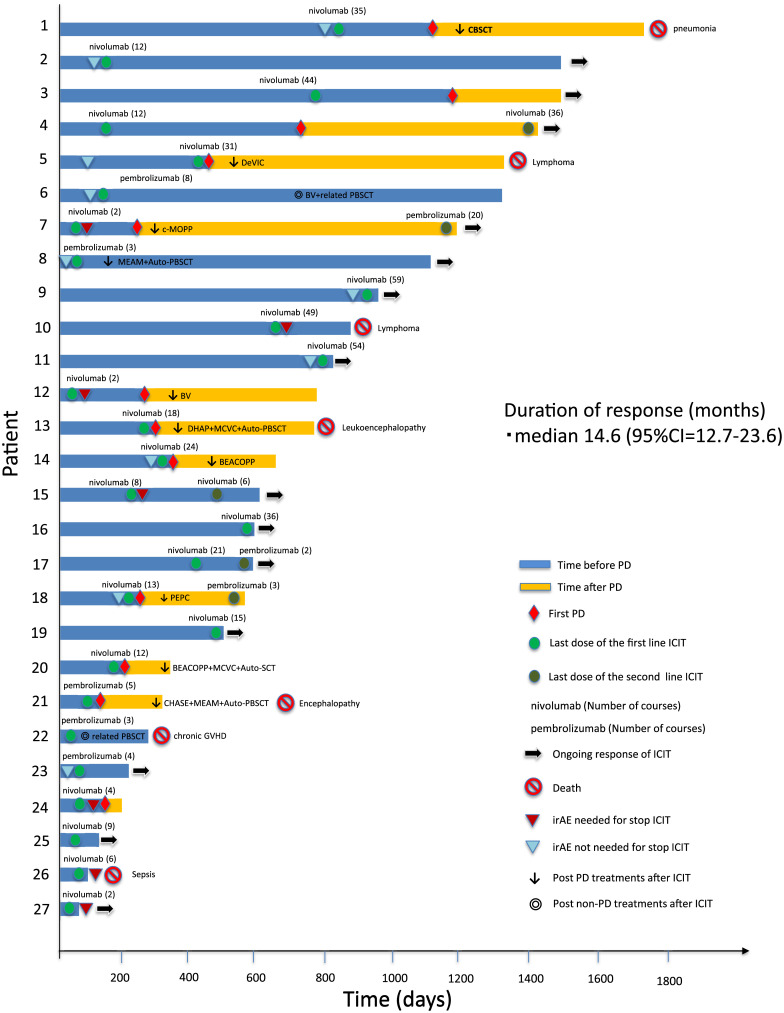
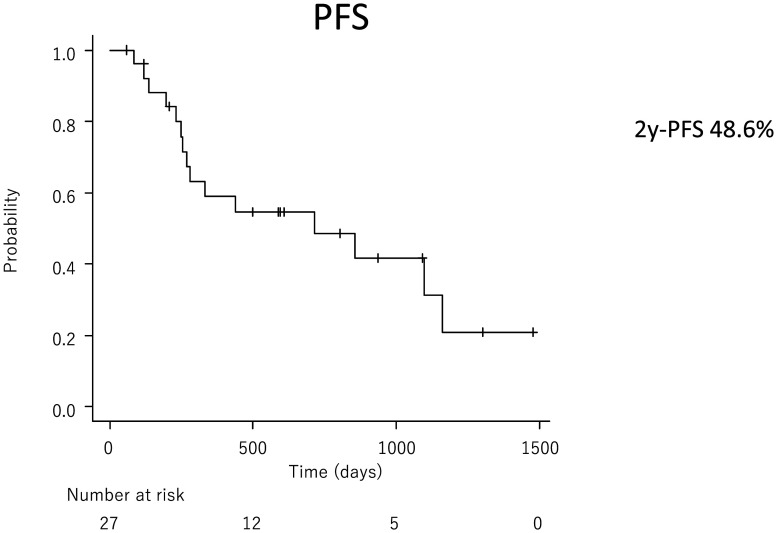
Immune checkpoint inhibitors (ICI) are promising therapeutic agents for relapsed or refractory classical Hodgkin's lymphoma (RRcHL). This retrospective study evaluated patients with RRcHL registered in the clinical research program Tohoku-Hematology-Forum-26, between 2016 and 2020, and treated with ICI in 14 centers in Northeast Japan. We analyzed the usage, efficacy, and safety of ICI therapy (ICIT). Among a total of 27 patients with RRcHL, 21 and nine were treated with nivolumab and/or pembrolizumab, respectively. The best response was complete response (CR), partial response (PR), stable disease (SD), and progressive disease in 11 (40.8%), seven (25.9%), eight (29.6%), and one (3.7%) patient, respectively. In all patients undergoing ICIT, the 2-year progression-free survival and 2-year overall survival (OS) were 48.6% and 87.4%, respectively. The 2-year OS for patients with CR, PR, and SD were 100%, 68.6%, and 87.5%, respectively. A total of 36 events of immune-related adverse events (irAEs) or immune-related like adverse events (irlAEs) were observed in 19 of the 27 patients (70.4%). Two thirds of these irAEs or irlAEs were grade 1-2 and controllable. During the observation period, ICIT was discontinued in 22 of 27 (81.4%) patients due to CR, inadequate response, irAE and patient circumstances in five (22.7%), seven (31.8%), eight (36.4%) and two patients (9.1%), respectively. Therapy-related mortality-associated irAE were observed in only one patient during ICIT. These results suggest that ICIT for RRcHL is effective and safe in real-world settings. The optimal timing of induction and duration of ICIT remains to be established.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
