Marie Dam Lauridsen , Simon Grøntved , Emil Fosbøl , Søren P. Johnsen , Jennifer K. Quint , Ulla Møller Weinreich , Jan Brink Valentin
{"title":"Treatment intensity level as a proxy for severity of chronic obstructive pulmonary disease: A risk stratification tool","authors":"Marie Dam Lauridsen , Simon Grøntved , Emil Fosbøl , Søren P. Johnsen , Jennifer K. Quint , Ulla Møller Weinreich , Jan Brink Valentin","doi":"10.1016/j.rmed.2024.107742","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Increasing severity of chronic obstructive pulmonary disease (COPD) is associated with increasing risk of poor outcomes. Using health registry data, we aimed to assess the association between treatment intensity levels (TIL), as a proxy for underlying COPD severity, and long-term outcomes.</p></div><div><h3>Methods</h3><p>Using Danish nationwide registries, we identified patients diagnosed with COPD during 2001–2016, who were alive at index date of 1 January 2017. We stratified patients into exclusive TILs from least to most severe: no use, short term therapy, mono-, dual-, triple therapy, oral corticosteroid (OCS), and long-term oxygen treatment (LTOT). Survival analyses were used to assess 5-year outcomes by TIL.</p></div><div><h3>Results</h3><p>We identified 53,803 patients with COPD in the study period (median age: 72 years [inter quartile range, 64–80], 48 % male). The three most severe TILs were associated with a significant incremental increase in all-cause mortality with an adjusted hazard ratio (aHR) for triple therapy, OCS and LTOT of 1.44 (95 % CI: 1.38–1.51), 1.67 (95 % CI: 1.59–1.75), and 2.91 (95 % CI: 2.76–3.07) compared with those receiving no therapy as reference. The same pattern was evident for the composite outcome of 5-year mortality or COPD-related hospitalization with an aHR for triple therapy, OCS and LTOT of 2.30 (95 % CI: 2.22–2.38), 2.85 (95 % CI: 2.74–2.96), and 4.00 (95 % CI: 3.81–4.20), respectively.</p></div><div><h3>Conclusion</h3><p>Increasing TILs were associated with increasing five-year mortality and risk of COPD-related hospitalization. TILs may be used as a proxy for underlying COPD severity in epidemiological studies.</p></div>","PeriodicalId":21057,"journal":{"name":"Respiratory medicine","volume":"232 ","pages":"Article 107742"},"PeriodicalIF":3.1000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Respiratory medicine","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0954611124002178","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/31 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
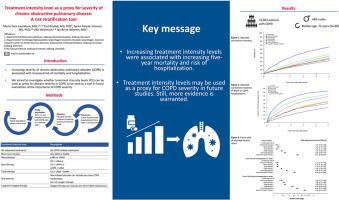
Increasing severity of chronic obstructive pulmonary disease (COPD) is associated with increasing risk of poor outcomes. Using health registry data, we aimed to assess the association between treatment intensity levels (TIL), as a proxy for underlying COPD severity, and long-term outcomes.
Methods
Using Danish nationwide registries, we identified patients diagnosed with COPD during 2001–2016, who were alive at index date of 1 January 2017. We stratified patients into exclusive TILs from least to most severe: no use, short term therapy, mono-, dual-, triple therapy, oral corticosteroid (OCS), and long-term oxygen treatment (LTOT). Survival analyses were used to assess 5-year outcomes by TIL.
Results
We identified 53,803 patients with COPD in the study period (median age: 72 years [inter quartile range, 64–80], 48 % male). The three most severe TILs were associated with a significant incremental increase in all-cause mortality with an adjusted hazard ratio (aHR) for triple therapy, OCS and LTOT of 1.44 (95 % CI: 1.38–1.51), 1.67 (95 % CI: 1.59–1.75), and 2.91 (95 % CI: 2.76–3.07) compared with those receiving no therapy as reference. The same pattern was evident for the composite outcome of 5-year mortality or COPD-related hospitalization with an aHR for triple therapy, OCS and LTOT of 2.30 (95 % CI: 2.22–2.38), 2.85 (95 % CI: 2.74–2.96), and 4.00 (95 % CI: 3.81–4.20), respectively.
Conclusion
Increasing TILs were associated with increasing five-year mortality and risk of COPD-related hospitalization. TILs may be used as a proxy for underlying COPD severity in epidemiological studies.
期刊介绍:
Respiratory Medicine is an internationally-renowned journal devoted to the rapid publication of clinically-relevant respiratory medicine research. It combines cutting-edge original research with state-of-the-art reviews dealing with all aspects of respiratory diseases and therapeutic interventions. Topics include adult and paediatric medicine, epidemiology, immunology and cell biology, physiology, occupational disorders, and the role of allergens and pollutants.
Respiratory Medicine is increasingly the journal of choice for publication of phased trial work, commenting on effectiveness, dosage and methods of action.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
