{"title":"Pharmacogenomic Prescribing Guidelines: Are They Always Useful?","authors":"Magnus Ingelman-Sundberg","doi":"10.1002/cpt.3403","DOIUrl":null,"url":null,"abstract":"<p>\n <b>An extensive review of the literature exploring the relationship between beta-blocker response and genetic variants associated with six polymorphic genes, culminating in a comprehensive guideline exceeding 130 pages for the clinical use of beta-blockers, is published in this issue of CPT. However, the authors found no genetically related significant effects warranting clinical guidance. This commentary questions the necessity of pharmacogenomic guidelines in such instances and advocates for shorter targeted easily understandable guidelines focused on phenotypes with clear clinical relevance useful in various healthcare settings.</b>\n </p><p>Pharmacogenomics is still largely in its infancy. Currently, we possess only about 30–40% understanding of the genetic inheritance basis relevant to pharmacogenomics. Many rare diseases are caused by mutations in regulatory gene regions, and recent evidence shows that a significant portion of important SNP-dependent regulation of clinically important CYPs is located within a 1 Mb distance from the gene. This indicates that much more information is required before we can enhance the clinical applicability of pharmacogenomic predictions.</p><p>In oncology, our knowledge of clinically meaningful pharmacogenomic applications for predicting drug response is more advanced. However, in other areas such as cardiovascular disease, the gene–drug pair clopidogrel-CYP2C19 is one of the few with some, albeit limited, clinical utilities.<span><sup>1, 2</sup></span>\n </p><p>In the study by Duarte et al.,<span><sup>3</sup></span> the authors conducted a thorough and high-quality literature investigation of the relationship between beta-blocker exposure and response in relation to the distribution of genetic variants of <i>CYP2D6, ADRB1, ADRB2, ADRA2C, GRK4</i>, and <i>GRK5</i>. Their survey found that after treatment with metoprolol, a decrease in heart rate by 3–8 beats per minute more in CYP2D6-PMs than in CYP2D6-NMs appeared to occur, whereas no significant CYP2D6-related effects were observed after treatment with other beta-blockers such as carvedilol, propranolol, labetalol, and nebivolol. On this basis, the authors provide an extensive guideline with therapeutic recommendations regarding the genetically predicted CYP2D6 metabolizer status and metoprolol therapy.</p><p>This raises questions about the cost–benefit impact of pharmacogenomic guidelines on clinical practice and metoprolol treatment in particular. The value of pharmacogenomics lies in identifying relevant gene–drug pairs where genetic variants cause clinically significant interindividual differences in drug response and side effects. When these pairs are clinically applicable and beneficial for patients, regulatory guidelines are essential to assist healthcare providers. However, in the case of beta-blocker action, such relationships are virtually absent,<span><sup>4-6</sup></span> making regulatory guidelines of less importance. The observed effects on heart rate (a reduction of 3–8 beats per minute) do not justify preemptive genetic testing. Consequently, in general guideline publications would only be produced when the accumulated evidence in the literature is sufficiently relevant to clinical practice and includes precise recommendations that need to be implemented.</p><p>The dissemination of guidelines without significant clinical applications may in fact cause less attention of the clinicians for using pharmacogenomics in health care. Healthcare providers might consider such guidelines as an administrative burden, which would diminish their interest in pharmacogenomic information in other therapeutic areas. It is therefore necessary to adapt the content of the guidelines to the clinical situation and to focus only on what is highly relevant for use in the clinics.</p><p>Pharmacogenomic recommendations are included in the product descriptions (e.g., drug labels, or summary of product characteristics (SmPCs). These recommendations are made by regulatory authorities such as the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA). In addition, academic organizations such as the Clinical Pharmacogenetics Implementation Consortium (CPIC) and the Dutch Pharmacogenetics Working Group (DPWG) provide guidelines of very high quality based on a lot of effort and knowledge among the experts involved for the use of drugs affected by genetic variants. In a comparison published in 2020 of the pharmacogenomic guidelines of the FDA and various European authorities, including the EMA, as well as the University ter Beoordeling van Geneesmiddelen Medicines Evaluation Board (CBG-MEB) and the Federal Institute for Drugs and Medical Devices (FIDMD) for drugs authorized before the establishment of the EMA in 1995 (collectively referred to as EMA/FM), we found notable discrepancies.<span><sup>7</sup></span> Similar heterogeneities in guideline data have also been published by Koutsilieri et al.<span><sup>8</sup></span>\n </p><p>We examined the pharmacogenomic labelling information on 505 different drugs provided by the CPIC, DPWG, FDA, and EMA/FM.<span><sup>6</sup></span> Of the 54 drugs with actionable gene–drug interactions according to CPIC and DPWG guidelines, only 50% of the corresponding SmPCs or drug labelling contained actionable pharmacogenomic information. Concordant FDA, EMA/FM, CPIC, and DPWG recommendations were found for only 10 (18%) of these 54 drugs. In addition, we examined 450 additional drugs for which there are no CPIC or DPWG recommendations and identified 126 with actionable genetics labelling according to the FDA and/or EMA/FM. For these 126 drugs and the 54 original drugs, the agreement between the FDA and EMA/FM for usable pharmacogenomic labelling was only 54%.</p><p>These discrepancies weaken the clinical importance of pharmacogenomic counseling. This is mainly because the scientific and clinical basis for many of the studies published is weak. These problems could be related to (i) underpowered studies, (ii) irrelevant selection of drug-gene pairs studied, (iii) open-label clinical trials causing significant placebo effects, (iv) heterogeneous disease classification, and (v) insufficient number of studies. As a result, many of the conclusions raised are not reproducible. In addition, many meta-analyses in this area are not homogeneous enough, for example, in terms of (i) drug concentrations, (ii) drug selection, (iii) timing of treatment, and (iv) initial pathophysiological definition (cf. ref. [<span>9</span>]). It is clear that more meaningful and stratified clinical trials should lead to a greater consensus between authorities, which would significantly improve the implementation of pharmacogenomic drug labelling in clinical practice.</p><p>According to my opinion, predictive pharmacogenomics should only be used if the gene–drug pair is well defined and the effects of gene variation at therapeutic concentrations are known to be clinically relevant. In this regard, the FDA has an interesting website<span><sup>10</sup></span> where gene–drug pairs with pharmacogenetic associations related to (i) therapeutic management recommendations, (ii) effects on safety or response, and (iii) effects on pharmacokinetic properties are listed. These pharmacogenomic associations provided by the FDA relate to gene variants of enzymes that metabolize drugs, to gene transporters, and to gene variants that have been associated with a predisposition to certain adverse events. Interestingly, 70% of the 124 pharmacogenomic biomarkers in Group 1) are related to genetic variations only in the <i>CYP2C9, CYP2C19</i>, or <i>CYP2D6</i> genes and 63% of the biomarkers are related to the CNS or oncology therapeutic areas and only propafenone and warfarin to the cardiovascular area. The FDA-approved metoprolol label does not contain any recommendations on pharmacogenomics.<span><sup>11</sup></span>\n </p><p>For scientists in the field of pharmacogenomics, it is obvious that the use of pharmacogenomic information in routine clinical practice is underdeveloped or underutilized in most European and American countries. Clear, concise guidelines aimed more at clinicians in routine care would improve implementation in the future. In this context, it is important to limit these guidelines to cases where the genetic aspect is indeed substantial compared with other factors influencing interindividual variability in drug response and adverse events are used, that is, to focus only on relevant genetic variants causing a PM or a UM phenotype (see <b>Figure</b> \n <b>1</b>\n ).</p><p>Many of the pharmacogenomic guidelines that have been produced are very extensive and run to many pages. They are mainly aimed at professionals in the field, many of them in the biotech industry as stakeholders in the field. However, as mentioned, there is a lack of guidelines with a purely clinical profile covering the most important parts of pharmacogenomics in different therapeutic areas. It can be argued that producing guidelines that require a huge amount of work and focus on drug therapies with limited or no clinical relevance would be a waste of time. However, future targeted guidelines, developed in close collaboration with physicians in the different therapeutic areas and regularly updated, would benefit the implementation of pharmacogenomics in health care and lead to more cost-effective and better-individualized pharmacotherapy.</p><p>No funding was received for this work.</p><p>Magnus Ingelman-Sundberg is a co-founder and shareholder of HepaPredict AB.</p>","PeriodicalId":153,"journal":{"name":"Clinical Pharmacology & Therapeutics","volume":"116 4","pages":"899-901"},"PeriodicalIF":5.5000,"publicationDate":"2024-08-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cpt.3403","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacology & Therapeutics","FirstCategoryId":"3","ListUrlMain":"https://ascpt.onlinelibrary.wiley.com/doi/10.1002/cpt.3403","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
An extensive review of the literature exploring the relationship between beta-blocker response and genetic variants associated with six polymorphic genes, culminating in a comprehensive guideline exceeding 130 pages for the clinical use of beta-blockers, is published in this issue of CPT. However, the authors found no genetically related significant effects warranting clinical guidance. This commentary questions the necessity of pharmacogenomic guidelines in such instances and advocates for shorter targeted easily understandable guidelines focused on phenotypes with clear clinical relevance useful in various healthcare settings.
Pharmacogenomics is still largely in its infancy. Currently, we possess only about 30–40% understanding of the genetic inheritance basis relevant to pharmacogenomics. Many rare diseases are caused by mutations in regulatory gene regions, and recent evidence shows that a significant portion of important SNP-dependent regulation of clinically important CYPs is located within a 1 Mb distance from the gene. This indicates that much more information is required before we can enhance the clinical applicability of pharmacogenomic predictions.
In oncology, our knowledge of clinically meaningful pharmacogenomic applications for predicting drug response is more advanced. However, in other areas such as cardiovascular disease, the gene–drug pair clopidogrel-CYP2C19 is one of the few with some, albeit limited, clinical utilities.1, 2
In the study by Duarte et al.,3 the authors conducted a thorough and high-quality literature investigation of the relationship between beta-blocker exposure and response in relation to the distribution of genetic variants of CYP2D6, ADRB1, ADRB2, ADRA2C, GRK4, and GRK5. Their survey found that after treatment with metoprolol, a decrease in heart rate by 3–8 beats per minute more in CYP2D6-PMs than in CYP2D6-NMs appeared to occur, whereas no significant CYP2D6-related effects were observed after treatment with other beta-blockers such as carvedilol, propranolol, labetalol, and nebivolol. On this basis, the authors provide an extensive guideline with therapeutic recommendations regarding the genetically predicted CYP2D6 metabolizer status and metoprolol therapy.
This raises questions about the cost–benefit impact of pharmacogenomic guidelines on clinical practice and metoprolol treatment in particular. The value of pharmacogenomics lies in identifying relevant gene–drug pairs where genetic variants cause clinically significant interindividual differences in drug response and side effects. When these pairs are clinically applicable and beneficial for patients, regulatory guidelines are essential to assist healthcare providers. However, in the case of beta-blocker action, such relationships are virtually absent,4-6 making regulatory guidelines of less importance. The observed effects on heart rate (a reduction of 3–8 beats per minute) do not justify preemptive genetic testing. Consequently, in general guideline publications would only be produced when the accumulated evidence in the literature is sufficiently relevant to clinical practice and includes precise recommendations that need to be implemented.
The dissemination of guidelines without significant clinical applications may in fact cause less attention of the clinicians for using pharmacogenomics in health care. Healthcare providers might consider such guidelines as an administrative burden, which would diminish their interest in pharmacogenomic information in other therapeutic areas. It is therefore necessary to adapt the content of the guidelines to the clinical situation and to focus only on what is highly relevant for use in the clinics.
Pharmacogenomic recommendations are included in the product descriptions (e.g., drug labels, or summary of product characteristics (SmPCs). These recommendations are made by regulatory authorities such as the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA). In addition, academic organizations such as the Clinical Pharmacogenetics Implementation Consortium (CPIC) and the Dutch Pharmacogenetics Working Group (DPWG) provide guidelines of very high quality based on a lot of effort and knowledge among the experts involved for the use of drugs affected by genetic variants. In a comparison published in 2020 of the pharmacogenomic guidelines of the FDA and various European authorities, including the EMA, as well as the University ter Beoordeling van Geneesmiddelen Medicines Evaluation Board (CBG-MEB) and the Federal Institute for Drugs and Medical Devices (FIDMD) for drugs authorized before the establishment of the EMA in 1995 (collectively referred to as EMA/FM), we found notable discrepancies.7 Similar heterogeneities in guideline data have also been published by Koutsilieri et al.8
We examined the pharmacogenomic labelling information on 505 different drugs provided by the CPIC, DPWG, FDA, and EMA/FM.6 Of the 54 drugs with actionable gene–drug interactions according to CPIC and DPWG guidelines, only 50% of the corresponding SmPCs or drug labelling contained actionable pharmacogenomic information. Concordant FDA, EMA/FM, CPIC, and DPWG recommendations were found for only 10 (18%) of these 54 drugs. In addition, we examined 450 additional drugs for which there are no CPIC or DPWG recommendations and identified 126 with actionable genetics labelling according to the FDA and/or EMA/FM. For these 126 drugs and the 54 original drugs, the agreement between the FDA and EMA/FM for usable pharmacogenomic labelling was only 54%.
These discrepancies weaken the clinical importance of pharmacogenomic counseling. This is mainly because the scientific and clinical basis for many of the studies published is weak. These problems could be related to (i) underpowered studies, (ii) irrelevant selection of drug-gene pairs studied, (iii) open-label clinical trials causing significant placebo effects, (iv) heterogeneous disease classification, and (v) insufficient number of studies. As a result, many of the conclusions raised are not reproducible. In addition, many meta-analyses in this area are not homogeneous enough, for example, in terms of (i) drug concentrations, (ii) drug selection, (iii) timing of treatment, and (iv) initial pathophysiological definition (cf. ref. [9]). It is clear that more meaningful and stratified clinical trials should lead to a greater consensus between authorities, which would significantly improve the implementation of pharmacogenomic drug labelling in clinical practice.
According to my opinion, predictive pharmacogenomics should only be used if the gene–drug pair is well defined and the effects of gene variation at therapeutic concentrations are known to be clinically relevant. In this regard, the FDA has an interesting website10 where gene–drug pairs with pharmacogenetic associations related to (i) therapeutic management recommendations, (ii) effects on safety or response, and (iii) effects on pharmacokinetic properties are listed. These pharmacogenomic associations provided by the FDA relate to gene variants of enzymes that metabolize drugs, to gene transporters, and to gene variants that have been associated with a predisposition to certain adverse events. Interestingly, 70% of the 124 pharmacogenomic biomarkers in Group 1) are related to genetic variations only in the CYP2C9, CYP2C19, or CYP2D6 genes and 63% of the biomarkers are related to the CNS or oncology therapeutic areas and only propafenone and warfarin to the cardiovascular area. The FDA-approved metoprolol label does not contain any recommendations on pharmacogenomics.11
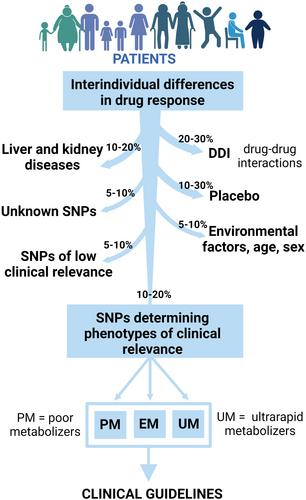
For scientists in the field of pharmacogenomics, it is obvious that the use of pharmacogenomic information in routine clinical practice is underdeveloped or underutilized in most European and American countries. Clear, concise guidelines aimed more at clinicians in routine care would improve implementation in the future. In this context, it is important to limit these guidelines to cases where the genetic aspect is indeed substantial compared with other factors influencing interindividual variability in drug response and adverse events are used, that is, to focus only on relevant genetic variants causing a PM or a UM phenotype (see Figure1
).
Many of the pharmacogenomic guidelines that have been produced are very extensive and run to many pages. They are mainly aimed at professionals in the field, many of them in the biotech industry as stakeholders in the field. However, as mentioned, there is a lack of guidelines with a purely clinical profile covering the most important parts of pharmacogenomics in different therapeutic areas. It can be argued that producing guidelines that require a huge amount of work and focus on drug therapies with limited or no clinical relevance would be a waste of time. However, future targeted guidelines, developed in close collaboration with physicians in the different therapeutic areas and regularly updated, would benefit the implementation of pharmacogenomics in health care and lead to more cost-effective and better-individualized pharmacotherapy.
No funding was received for this work.
Magnus Ingelman-Sundberg is a co-founder and shareholder of HepaPredict AB.
期刊介绍:
Clinical Pharmacology & Therapeutics (CPT) is the authoritative cross-disciplinary journal in experimental and clinical medicine devoted to publishing advances in the nature, action, efficacy, and evaluation of therapeutics. CPT welcomes original Articles in the emerging areas of translational, predictive and personalized medicine; new therapeutic modalities including gene and cell therapies; pharmacogenomics, proteomics and metabolomics; bioinformation and applied systems biology complementing areas of pharmacokinetics and pharmacodynamics, human investigation and clinical trials, pharmacovigilence, pharmacoepidemiology, pharmacometrics, and population pharmacology.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
