Arjen J. G. Meewisse, Annerixt Gribnau, Steven E. Thiessen, Dirk Jan Stenvers, Jeroen Hermanides, Mark L. van Zuylen
{"title":"Effect of time of day on outcomes in elective surgery: a systematic review","authors":"Arjen J. G. Meewisse, Annerixt Gribnau, Steven E. Thiessen, Dirk Jan Stenvers, Jeroen Hermanides, Mark L. van Zuylen","doi":"10.1111/anae.16395","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>The timing of elective surgery could affect clinical outcome because of diurnal rhythms of patient physiology as well as surgical team performance. Waiting times for elective surgery are increasing in many countries, leading to increasing interest in undertaking elective surgery in the evening or at night. We aimed to systematically review the literature on the effect of the timing of elective (but not urgent or emergency) surgery on mortality, morbidity and other clinical outcomes.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We searched databases for relevant studies combining the terms ‘circadian rhythm’ and ‘anaesthesia/surgery’. Additional relevant articles were found by hand-searching the references. All studies were screened for bias. Included studies examined daytime vs. evening/night-time surgery, morning vs. afternoon surgery, multiple timeslots or used time as a continuous variable.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Nineteen retrospective cohort studies, one prospective cohort study and one randomised controlled trial were included (n = 798,914). Evening/night-time elective surgery was associated with a higher risk of mortality when compared with daytime procedures in three studies (n = 611,230), with odds ratios (95%CI) for mortality ranging from 1.35 (1.16–1.56) to 3.98 (1.54–10.30), while no differences were found in three other studies (n = 142,355). No differences were found for morning vs. afternoon surgery (four studies, n = 3277). However, most studies had a low quality of evidence due to their retrospective nature and because not all studies corrected for patient characteristics. Moreover, the studies were heterogeneous in terms of the reported time slots and clinical outcomes.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>We found that evening/night-time elective surgery is associated with a higher risk of mortality compared with daytime surgery. However, the quality of evidence was graded as low, and thus, future prospective research should publish individual patient data and standardise outcome measures to allow firm conclusions and facilitate interventions.</p>\n </section>\n </div>","PeriodicalId":7742,"journal":{"name":"Anaesthesia","volume":"79 12","pages":"1325-1334"},"PeriodicalIF":6.9000,"publicationDate":"2024-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/anae.16395","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anaesthesia","FirstCategoryId":"3","ListUrlMain":"https://associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/10.1111/anae.16395","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
The timing of elective surgery could affect clinical outcome because of diurnal rhythms of patient physiology as well as surgical team performance. Waiting times for elective surgery are increasing in many countries, leading to increasing interest in undertaking elective surgery in the evening or at night. We aimed to systematically review the literature on the effect of the timing of elective (but not urgent or emergency) surgery on mortality, morbidity and other clinical outcomes.
Methods
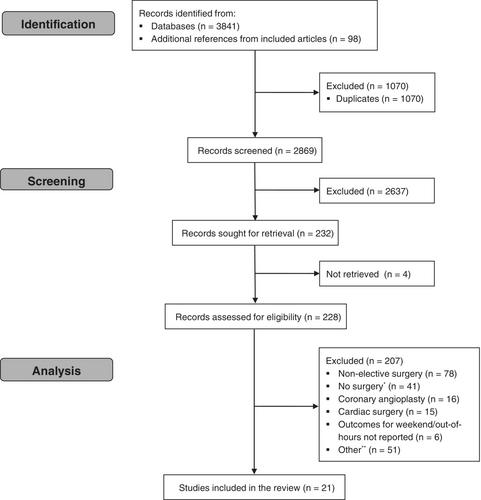
We searched databases for relevant studies combining the terms ‘circadian rhythm’ and ‘anaesthesia/surgery’. Additional relevant articles were found by hand-searching the references. All studies were screened for bias. Included studies examined daytime vs. evening/night-time surgery, morning vs. afternoon surgery, multiple timeslots or used time as a continuous variable.
Results
Nineteen retrospective cohort studies, one prospective cohort study and one randomised controlled trial were included (n = 798,914). Evening/night-time elective surgery was associated with a higher risk of mortality when compared with daytime procedures in three studies (n = 611,230), with odds ratios (95%CI) for mortality ranging from 1.35 (1.16–1.56) to 3.98 (1.54–10.30), while no differences were found in three other studies (n = 142,355). No differences were found for morning vs. afternoon surgery (four studies, n = 3277). However, most studies had a low quality of evidence due to their retrospective nature and because not all studies corrected for patient characteristics. Moreover, the studies were heterogeneous in terms of the reported time slots and clinical outcomes.
Conclusions
We found that evening/night-time elective surgery is associated with a higher risk of mortality compared with daytime surgery. However, the quality of evidence was graded as low, and thus, future prospective research should publish individual patient data and standardise outcome measures to allow firm conclusions and facilitate interventions.
期刊介绍:
The official journal of the Association of Anaesthetists is Anaesthesia. It is a comprehensive international publication that covers a wide range of topics. The journal focuses on general and regional anaesthesia, as well as intensive care and pain therapy. It includes original articles that have undergone peer review, covering all aspects of these fields, including research on equipment.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
