Rebecca Ohman-Hanson, G. Todd Alonso, Laura Pyle, Ryan McDonough, Mark Clements
{"title":"Management of diabetic ketoacidosis in children: Does early insulin glargine help improve outcomes?","authors":"Rebecca Ohman-Hanson, G. Todd Alonso, Laura Pyle, Ryan McDonough, Mark Clements","doi":"10.1111/1753-0407.13597","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Rebound hyperglycemia following the resolution of diabetic ketoacidosis (DKA) is common in pediatric patients with type 1 diabetes, increasing the risk of recurrent DKA and complicating the transition to subcutaneous insulin. Multiple studies suggest that early administration of long-acting insulin analogs during DKA management safely improves this transition.</p>\n </section>\n \n <section>\n \n <h3> Objective</h3>\n \n <p>This study aimed to determine whether early insulin glargine administration in children with DKA prevents rebound hyperglycemia and recurrent ketosis without increasing the rate of hypoglycemia or hypokalemia.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Patients aged <21 years presenting with DKA to Children's Mercy Kansas City between October 2012 and October 2016 were reviewed. They were categorized as Early (>4 h of overlap with intravenous [IV] insulin) and Late (<2 h of overlap) cohorts.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>We reviewed 546 DKA admissions (365 Early and 181 Late). Rebound hyperglycemia (>180 mg/dL) was lower in the Early group (66% vs. 85%, <i>p</i> ≤ 0.0001). Hypoglycemia (<70 mg/dL) during IV insulin administration was higher in the Early group than in the Late group (27% vs. 19%, <i>p</i> = 0.042). Hypoglycemia within 12 h of IV insulin discontinuation was lower in the Early group (16% vs. 26%, <i>p</i> = 0.012). Recurrent ketosis, hypokalemia, and cerebral edema were not different between the groups.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Early glargine administration in pediatric DKA management is safe, decreases the rate of rebound hyperglycemia, and improves the transition to subcutaneous insulin. Hypoglycemia is less frequent following IV insulin discontinuation with early glargine, but the IV insulin rate may need to be reduced to minimize hypoglycemia during IV insulin infusion.</p>\n \n <div>\n <figure>\n <div><picture>\n <source></source></picture><p></p>\n </div>\n </figure>\n </div>\n </section>\n </div>","PeriodicalId":189,"journal":{"name":"Journal of Diabetes","volume":"16 8","pages":""},"PeriodicalIF":3.0000,"publicationDate":"2024-08-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1753-0407.13597","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Diabetes","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/1753-0407.13597","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Rebound hyperglycemia following the resolution of diabetic ketoacidosis (DKA) is common in pediatric patients with type 1 diabetes, increasing the risk of recurrent DKA and complicating the transition to subcutaneous insulin. Multiple studies suggest that early administration of long-acting insulin analogs during DKA management safely improves this transition.
Objective
This study aimed to determine whether early insulin glargine administration in children with DKA prevents rebound hyperglycemia and recurrent ketosis without increasing the rate of hypoglycemia or hypokalemia.
Methods
Patients aged <21 years presenting with DKA to Children's Mercy Kansas City between October 2012 and October 2016 were reviewed. They were categorized as Early (>4 h of overlap with intravenous [IV] insulin) and Late (<2 h of overlap) cohorts.
Results
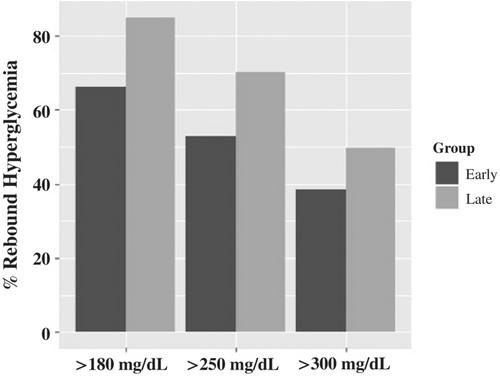
We reviewed 546 DKA admissions (365 Early and 181 Late). Rebound hyperglycemia (>180 mg/dL) was lower in the Early group (66% vs. 85%, p ≤ 0.0001). Hypoglycemia (<70 mg/dL) during IV insulin administration was higher in the Early group than in the Late group (27% vs. 19%, p = 0.042). Hypoglycemia within 12 h of IV insulin discontinuation was lower in the Early group (16% vs. 26%, p = 0.012). Recurrent ketosis, hypokalemia, and cerebral edema were not different between the groups.
Conclusions
Early glargine administration in pediatric DKA management is safe, decreases the rate of rebound hyperglycemia, and improves the transition to subcutaneous insulin. Hypoglycemia is less frequent following IV insulin discontinuation with early glargine, but the IV insulin rate may need to be reduced to minimize hypoglycemia during IV insulin infusion.
期刊介绍:
Journal of Diabetes (JDB) devotes itself to diabetes research, therapeutics, and education. It aims to involve researchers and practitioners in a dialogue between East and West via all aspects of epidemiology, etiology, pathogenesis, management, complications and prevention of diabetes, including the molecular, biochemical, and physiological aspects of diabetes. The Editorial team is international with a unique mix of Asian and Western participation.
The Editors welcome submissions in form of original research articles, images, novel case reports and correspondence, and will solicit reviews, point-counterpoint, commentaries, editorials, news highlights, and educational content.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
