Intraoperative Detection of Extracochlear Electrodes Using Stimulation Current Induced Non-Stimulating Electrode Voltage (SCINSEV) Measures (Transimpedance Measures)—A Case Series
Muhammed Ayas, Yu Chuen Tam, Dakota Bysouth-Young, Susan T. Eitutis, Marina Salorio-Corbetto, Patrick R. Axon, Neil P. Donnelly, James R. Tysome, Daniele Borsetto, Mathew E. Smith, Manohar L. Bance
{"title":"Intraoperative Detection of Extracochlear Electrodes Using Stimulation Current Induced Non-Stimulating Electrode Voltage (SCINSEV) Measures (Transimpedance Measures)—A Case Series","authors":"Muhammed Ayas, Yu Chuen Tam, Dakota Bysouth-Young, Susan T. Eitutis, Marina Salorio-Corbetto, Patrick R. Axon, Neil P. Donnelly, James R. Tysome, Daniele Borsetto, Mathew E. Smith, Manohar L. Bance","doi":"10.1111/coa.14212","DOIUrl":null,"url":null,"abstract":"<p>Cochlear implants (CIs) are prosthetic devices used to restore hearing sensation in people with severe to profound sensorineural hearing loss [<span>1</span>]. The success of the CI surgery relies on the surgical placement of the electrodes within the scala tympani. Electrode migration post placement is well documented and could significantly affect the overall CI performance [<span>2</span>]. Migration may result in extracochlear electrodes (EE). Notably, this is under-reported in the existing literature [<span>3, 4</span>]. Routine intraoperative measures, such as contact impedances, may not indicate misplacement or extrusion of electrodes, particularly if there is an electrically conductive blood, fluid, or soft tissue around the EEs, which may result in the normal contact impedances. If the EE are in air, the contact impedances will show an open circuit and so are easier to detect [<span>5, 6</span>]. Advanced measures such as the stimulation current induced non-stimulating electrode voltage (SCINSEV- termed differently in various clinical software as transimpedance matrix (TIM) by Cochlear Corp, electric field imaging (EFI) by Advanced Bionics(AB) and impedance field telemetry (IFT) by MEDEL), could potentially be used to detect the extrusion EE. The application of SCINSEV measurements in cadaveric studies demonstrates a comparable and well-defined role in the identification of electrode EE, as detailed in the existing literature [<span>5, 6</span>]. Here, we report three cases of intraoperative electrode extrusion detected using SCINSEV measures, subsequently performing corrective repositioning during the same surgical session which prevented the need for delayed revision surgery. This report further highlights the potential of SCINSEV as an important tool in intraoperative measures and enhancing CI surgical outcomes and reports for the first time their use in live patient surgery as determinants of EE and for intraoperative decision-making and correction.</p><p>Three paediatric patients are reported, implanted either bilaterally or unilaterally on the basis of multidisciplinary team decisions. All the 3 patients were females, with a mean age of 11 ± 3 years (Table 1). Preoperative magnetic resonance imaging (MRI) was performed to evaluate cochlear anatomical structures and assess the integrity of the auditory nerve. All the patients were implanted with AB HiRes Ultra 3D implants using the round window approach. After periosteal closure, intraoperative electrical impedance and other measurements were performed.</p><p>In our centre, the intraoperative test protocol follows a battery of tests including initial contact impedance measures, subsequent SCINSEV (termed EFI by AB) and Electrical Compound Action Potentials (ECAP). Following CI placement in the subperiosteal pocket and electrode insertion, the external coil is attached underneath the sterile surgical drapes and connected to a AB-AIM (active insertion monitoring) tablet system, and SCINSEV recordings are analysed by EFI analysis tool version 1.2 software (this software, currently experimental on the AIM tablet, is not commercially available at the moment). In instances where SCINSEV measures yielded inconclusive results regarding the presence of EE, ECAP assessments were also used to make determinations, particularly those from the basal end of the electrode array. It is important to note again that the contact impedances by themselves are not sensitive for detection of EE if the electrodes are surrounded by blood, saline or soft-tissue [<span>5, 6</span>].</p><p>If ECAP responses were absent in basal electrodes, such as for electrodes 16 or 15 for AB electrode arrays, adjacent electrode ECAP measurement were examined to determine the first electrode where robust responses were obtained. The ECAP profiles were subsequently compared with SCINSEV data to make a definitive determination of EE, indicated by a decreased intracochlear electrode voltage profile at the basal end of the array in the absence of ECAP response for the most basal electrodes. Where EE were expected, the wound was reopened, and the electrode repositioned. The entire battery of tests was then repeated. Post-operative x-rays were performed for all the patients approximately two to three weeks later to check for extrusion of the electrode array. The study followed the CARE reporting guidelines [<span>7</span>].</p><p>In this report we presented three cases of intraoperative electrode extrusion that occurred after the operating surgeon felt that full insertion of the electrode had been achieved. Intraoperative SCINSEV measurements subsequently identified EE and allowed for surgical correction, thereby averting the need for basal electrode inactivation during programming or delayed revision surgery for electrode repositioning.</p><p>Electrode extrusion is an important factor that can significantly affect the overall outcome in the patients with CI [<span>8</span>]. A recently published report indicates that approximately 11.5% of CI recipients experience electrode extrusion of various numbers of electrodes within the first few weeks of post-surgery [<span>3</span>]. This is alarming, as it necessitates the deactivation of approximately one to two electrodes during the CI programming stage, thereby potentially limiting the overall benefits [<span>9</span>]. The effective application of SCINSEVs and timely intervention by the surgical team have proven to be a critical factor in immediate repositioning of the electrodes completely inside the cochlea in our three cases. In three cases, lack of ECAPs at the base might have led to suspicion and need for intraoperative x-ray, but the confirmatory SCINSEV avoided this.</p><p>The salient marker for EE in the three cases presented here are that they show a notable decline in the intracochlear voltage profile especially at the basal electrode array. This is in keeping with what has been previously described as the marker for EE in cadaveric models [<span>5, 6</span>] but not, to date, reported in living human subjects. The SCINSEV measurements depicted in the heat map and in the line graph are essentially generated after the transimpedance measures by removing the contact impedances and plotting the ‘tails’ of the transimpedance measure [<span>6, 10</span>]. They basically document the electric field generated by each individual stimulated electrode by measuring the voltage generated on every other electrode in the array. These are generally available in all the CI manufacturers' clinical software in different versions. This enables clinicians to identify both the presence, and often the number of electrodes that are outside the cochlea.</p><p>This study not only underscores the clinical significance of SCINSEV but also affirms its role as an important tool in intraoperative settings. Detecting and addressing the electrode extrusion during the same surgical session not only avoids radiation but also mitigates potential delays in waiting for radiographers. This could significantly enhance consistency and cost-effectiveness of CI surgical placement. Stimulation current induced non-stimulating electrode voltage measures from most companies take less than 5 min to perform and can be easily repeated for several times such as after insertion and after full closure of the wound. This might be useful, for instance if an electrode is felt to be unstable and shows tendencies for extrusion during the surgery.</p><p>This case series reports the use of SCINSEVs for the intraoperative detection and correction of EE in live human patients. It validates the important role of SCINSEV measurements in ensuring optimal electrode array placement intraoperatively. Importantly, employing SCINSEV measures intraoperatively not only facilitates the corrective repositioning of electrode arrays within the same session but may also enhance operational efficiency for theatre utilization as these measures are rapid and do not use x-ray resources. Our clinical experience leads us to recommend the routine use of these measures in all CI surgeries.</p><p>Muhammed Ayas, Manohar L Bance, Yu Cheun Tam designed the work. Muhammed Ayas acquired, analysed and drafted the manuscript. Yu Chuen Tam, Dakota Bysouth-Young, Susan T. Eitutis, Marina Salorio-Corbetto acquired the data, reviewed and provided critical revision of the manuscript. Patrick R. Axon, Manohar L. Bance, James R. Tysome, Neil P. Donnelly, Mathew E. Smith, Daniele Borsetto performed cochlear implant surgeries, reviewed and provided critical revision of the manuscript. The authors discussed the results and implications and commented on the work at all stages.</p><p>Dr. James Tysome is Editor-in-Chief and Dr. Smith, Matthew is AE of the journal and co-author of this article. They were excluded from the peer-review process and all the editorial decisions related to the acceptance and publication of this article.</p>","PeriodicalId":10431,"journal":{"name":"Clinical Otolaryngology","volume":"49 6","pages":"827-832"},"PeriodicalIF":1.5000,"publicationDate":"2024-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/coa.14212","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Otolaryngology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/coa.14212","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Cochlear implants (CIs) are prosthetic devices used to restore hearing sensation in people with severe to profound sensorineural hearing loss [1]. The success of the CI surgery relies on the surgical placement of the electrodes within the scala tympani. Electrode migration post placement is well documented and could significantly affect the overall CI performance [2]. Migration may result in extracochlear electrodes (EE). Notably, this is under-reported in the existing literature [3, 4]. Routine intraoperative measures, such as contact impedances, may not indicate misplacement or extrusion of electrodes, particularly if there is an electrically conductive blood, fluid, or soft tissue around the EEs, which may result in the normal contact impedances. If the EE are in air, the contact impedances will show an open circuit and so are easier to detect [5, 6]. Advanced measures such as the stimulation current induced non-stimulating electrode voltage (SCINSEV- termed differently in various clinical software as transimpedance matrix (TIM) by Cochlear Corp, electric field imaging (EFI) by Advanced Bionics(AB) and impedance field telemetry (IFT) by MEDEL), could potentially be used to detect the extrusion EE. The application of SCINSEV measurements in cadaveric studies demonstrates a comparable and well-defined role in the identification of electrode EE, as detailed in the existing literature [5, 6]. Here, we report three cases of intraoperative electrode extrusion detected using SCINSEV measures, subsequently performing corrective repositioning during the same surgical session which prevented the need for delayed revision surgery. This report further highlights the potential of SCINSEV as an important tool in intraoperative measures and enhancing CI surgical outcomes and reports for the first time their use in live patient surgery as determinants of EE and for intraoperative decision-making and correction.
Three paediatric patients are reported, implanted either bilaterally or unilaterally on the basis of multidisciplinary team decisions. All the 3 patients were females, with a mean age of 11 ± 3 years (Table 1). Preoperative magnetic resonance imaging (MRI) was performed to evaluate cochlear anatomical structures and assess the integrity of the auditory nerve. All the patients were implanted with AB HiRes Ultra 3D implants using the round window approach. After periosteal closure, intraoperative electrical impedance and other measurements were performed.
In our centre, the intraoperative test protocol follows a battery of tests including initial contact impedance measures, subsequent SCINSEV (termed EFI by AB) and Electrical Compound Action Potentials (ECAP). Following CI placement in the subperiosteal pocket and electrode insertion, the external coil is attached underneath the sterile surgical drapes and connected to a AB-AIM (active insertion monitoring) tablet system, and SCINSEV recordings are analysed by EFI analysis tool version 1.2 software (this software, currently experimental on the AIM tablet, is not commercially available at the moment). In instances where SCINSEV measures yielded inconclusive results regarding the presence of EE, ECAP assessments were also used to make determinations, particularly those from the basal end of the electrode array. It is important to note again that the contact impedances by themselves are not sensitive for detection of EE if the electrodes are surrounded by blood, saline or soft-tissue [5, 6].
If ECAP responses were absent in basal electrodes, such as for electrodes 16 or 15 for AB electrode arrays, adjacent electrode ECAP measurement were examined to determine the first electrode where robust responses were obtained. The ECAP profiles were subsequently compared with SCINSEV data to make a definitive determination of EE, indicated by a decreased intracochlear electrode voltage profile at the basal end of the array in the absence of ECAP response for the most basal electrodes. Where EE were expected, the wound was reopened, and the electrode repositioned. The entire battery of tests was then repeated. Post-operative x-rays were performed for all the patients approximately two to three weeks later to check for extrusion of the electrode array. The study followed the CARE reporting guidelines [7].
In this report we presented three cases of intraoperative electrode extrusion that occurred after the operating surgeon felt that full insertion of the electrode had been achieved. Intraoperative SCINSEV measurements subsequently identified EE and allowed for surgical correction, thereby averting the need for basal electrode inactivation during programming or delayed revision surgery for electrode repositioning.
Electrode extrusion is an important factor that can significantly affect the overall outcome in the patients with CI [8]. A recently published report indicates that approximately 11.5% of CI recipients experience electrode extrusion of various numbers of electrodes within the first few weeks of post-surgery [3]. This is alarming, as it necessitates the deactivation of approximately one to two electrodes during the CI programming stage, thereby potentially limiting the overall benefits [9]. The effective application of SCINSEVs and timely intervention by the surgical team have proven to be a critical factor in immediate repositioning of the electrodes completely inside the cochlea in our three cases. In three cases, lack of ECAPs at the base might have led to suspicion and need for intraoperative x-ray, but the confirmatory SCINSEV avoided this.
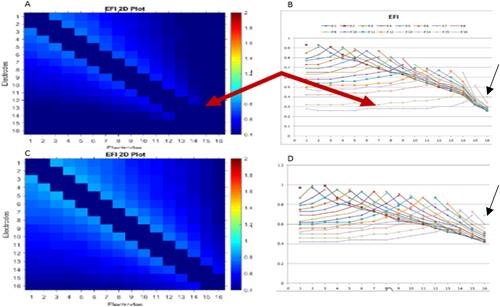
The salient marker for EE in the three cases presented here are that they show a notable decline in the intracochlear voltage profile especially at the basal electrode array. This is in keeping with what has been previously described as the marker for EE in cadaveric models [5, 6] but not, to date, reported in living human subjects. The SCINSEV measurements depicted in the heat map and in the line graph are essentially generated after the transimpedance measures by removing the contact impedances and plotting the ‘tails’ of the transimpedance measure [6, 10]. They basically document the electric field generated by each individual stimulated electrode by measuring the voltage generated on every other electrode in the array. These are generally available in all the CI manufacturers' clinical software in different versions. This enables clinicians to identify both the presence, and often the number of electrodes that are outside the cochlea.
This study not only underscores the clinical significance of SCINSEV but also affirms its role as an important tool in intraoperative settings. Detecting and addressing the electrode extrusion during the same surgical session not only avoids radiation but also mitigates potential delays in waiting for radiographers. This could significantly enhance consistency and cost-effectiveness of CI surgical placement. Stimulation current induced non-stimulating electrode voltage measures from most companies take less than 5 min to perform and can be easily repeated for several times such as after insertion and after full closure of the wound. This might be useful, for instance if an electrode is felt to be unstable and shows tendencies for extrusion during the surgery.
This case series reports the use of SCINSEVs for the intraoperative detection and correction of EE in live human patients. It validates the important role of SCINSEV measurements in ensuring optimal electrode array placement intraoperatively. Importantly, employing SCINSEV measures intraoperatively not only facilitates the corrective repositioning of electrode arrays within the same session but may also enhance operational efficiency for theatre utilization as these measures are rapid and do not use x-ray resources. Our clinical experience leads us to recommend the routine use of these measures in all CI surgeries.
Muhammed Ayas, Manohar L Bance, Yu Cheun Tam designed the work. Muhammed Ayas acquired, analysed and drafted the manuscript. Yu Chuen Tam, Dakota Bysouth-Young, Susan T. Eitutis, Marina Salorio-Corbetto acquired the data, reviewed and provided critical revision of the manuscript. Patrick R. Axon, Manohar L. Bance, James R. Tysome, Neil P. Donnelly, Mathew E. Smith, Daniele Borsetto performed cochlear implant surgeries, reviewed and provided critical revision of the manuscript. The authors discussed the results and implications and commented on the work at all stages.
Dr. James Tysome is Editor-in-Chief and Dr. Smith, Matthew is AE of the journal and co-author of this article. They were excluded from the peer-review process and all the editorial decisions related to the acceptance and publication of this article.
5% 的 CI 接受者在术后最初几周内会出现不同数量的电极挤压现象 [3]。这种情况令人担忧,因为这需要在 CI 编程阶段停用约一到两个电极,从而可能限制整体效益[9]。在我们的三个病例中,SCINSEVs 的有效应用和手术团队的及时干预已被证明是立即将电极完全重新定位在耳蜗内的关键因素。在这三个病例中,由于基底缺乏 ECAPs,可能会引起怀疑并需要术中进行 X 光检查,但 SCINSEV 的确认避免了这一情况的发生。在本文介绍的三个病例中,EE 的突出标志是耳蜗内电压曲线明显下降,尤其是在基底电极阵列处。这与之前在尸体模型[5, 6]中描述的 EE 标志一致,但迄今为止尚未在活人身上报道过。热图和折线图中描述的 SCINSEV 测量值基本上是在跨阻测量值之后通过去除接触阻抗和绘制跨阻测量值的 "尾部 "而产生的[6, 10]。它们基本上是通过测量阵列中每个其他电极上产生的电压来记录每个受刺激电极产生的电场。所有 CI 制造商的临床软件一般都有不同版本。这项研究不仅强调了 SCINSEV 的临床意义,还肯定了它作为术中重要工具的作用。在同一手术过程中检测和处理电极挤压不仅能避免辐射,还能减少等待放射技师的潜在延误。这将大大提高 CI 手术放置的一致性和成本效益。大多数公司提供的刺激电流诱导非刺激电极电压测量方法只需不到 5 分钟即可完成,而且可以轻松重复多次,例如在插入后和伤口完全闭合后。本病例系列报告了使用 SCINSEVs 在活体患者术中检测和纠正 EE 的情况。本病例系列报告了在活体患者术中使用 SCINSEV 检测和校正 EE 的情况,验证了 SCINSEV 测量在确保术中电极阵列最佳位置方面的重要作用。重要的是,在术中采用 SCINSEV 测量不仅有利于在同一疗程内对电极阵列进行纠正性重新定位,而且还能提高手术室的使用效率,因为这些测量既快速又不占用 X 射线资源。根据我们的临床经验,我们建议在所有 CI 手术中常规使用这些措施。Muhammed Ayas获取、分析并起草了手稿。Yu Chuen Tam、Dakota Bysouth-Young、Susan T. Eitutis、Marina Salorio-Corbetto获取数据、审阅并对手稿进行了重要修改。Patrick R. Axon、Manohar L. Bance、James R. Tysome、Neil P. Donnelly、Mathew E. Smith、Daniele Borsetto 进行了人工耳蜗植入手术,审阅并对手稿进行了重要修改。詹姆斯-泰索姆(James Tysome)博士是该杂志的主编,马修-史密斯(Mathew E. Smith)博士是该杂志的AE,也是本文的共同作者。詹姆斯-泰索姆博士是该期刊的主编,史密斯-马修博士是该期刊的助理编辑,也是本文的合著者。他们没有参与同行评审过程以及与接受和发表本文有关的所有编辑决策。
期刊介绍:
Clinical Otolaryngology is a bimonthly journal devoted to clinically-oriented research papers of the highest scientific standards dealing with:
current otorhinolaryngological practice
audiology, otology, balance, rhinology, larynx, voice and paediatric ORL
head and neck oncology
head and neck plastic and reconstructive surgery
continuing medical education and ORL training
The emphasis is on high quality new work in the clinical field and on fresh, original research.
Each issue begins with an editorial expressing the personal opinions of an individual with a particular knowledge of a chosen subject. The main body of each issue is then devoted to original papers carrying important results for those working in the field. In addition, topical review articles are published discussing a particular subject in depth, including not only the opinions of the author but also any controversies surrounding the subject.
• Negative/null results
In order for research to advance, negative results, which often make a valuable contribution to the field, should be published. However, articles containing negative or null results are frequently not considered for publication or rejected by journals. We welcome papers of this kind, where appropriate and valid power calculations are included that give confidence that a negative result can be relied upon.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
