Jeroen Deenik, Chris van Lieshout, Harold F van Driel, Geert W J Frederix, Ingrid J M Hendriksen, Peter N van Harten, Diederik E Tenback
{"title":"Cost-Effectiveness of a Multidisciplinary Lifestyle-Enhancing Treatment for Inpatients With Severe Mental Illness: The MULTI Study V.","authors":"Jeroen Deenik, Chris van Lieshout, Harold F van Driel, Geert W J Frederix, Ingrid J M Hendriksen, Peter N van Harten, Diederik E Tenback","doi":"10.1093/schizbullopen/sgac022","DOIUrl":null,"url":null,"abstract":"<p><p>Economic evaluations of lifestyle interventions for people with mental illness are needed to inform policymakers and managers about implementing such interventions and corresponding reforms in routine mental healthcare. We aimed to evaluate changes in healthcare costs 18 months after the implementation of a multidisciplinary lifestyle-enhancing treatment for inpatients with severe mental illness (MULTI) versus treatment as usual (TAU). In a cohort study (<i>n</i> = 114; 65 MULTI, 49 TAU), we retrospectively retrieved cost data in Euros on all patient sessions, ward stay, medication use, and hospital referrals in the quarter year at the start of MULTI (Q1 2014) and after its evaluation (Q3 2015). We used linear regression analyses correcting for baseline values and differences between groups, calculated deterministic incremental cost-effectiveness ratios for previously shown changes in physical activity, metabolic health, psychosocial functioning, and additionally quality of life, and performed probabilistic sensitivity analyses including cost-effectiveness planes. Adjusted regression showed reduced total costs per patient per quarter year in favor of MULTI (B = -736.30, 95%CI: -2145.2 to 672.6). Corresponding probabilistic sensitivity analyses accounting for uncertainty surrounding the parameters showed statistically non-significant cost savings against health improvements for all health-related outcomes in MULTI compared to TAU. It is concluded that MULTI did not increase healthcare costs while improving health outcomes. This indicates that starting lifestyle interventions does not need to be hampered by costs. Potential societal and economic value may justify investment to support implementation and maintenance. Further research is needed to study this hypothesis.</p>","PeriodicalId":94380,"journal":{"name":"Schizophrenia bulletin open","volume":"3 1","pages":"sgac022"},"PeriodicalIF":2.0000,"publicationDate":"2022-02-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11206082/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Schizophrenia bulletin open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/schizbullopen/sgac022","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
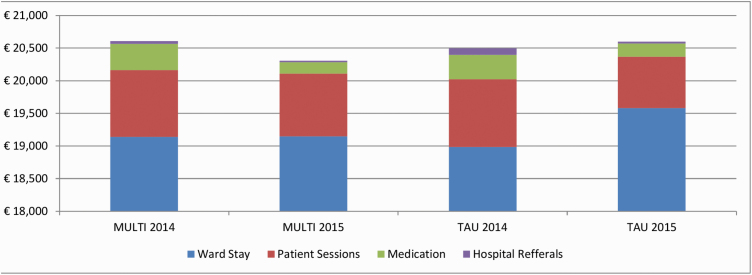
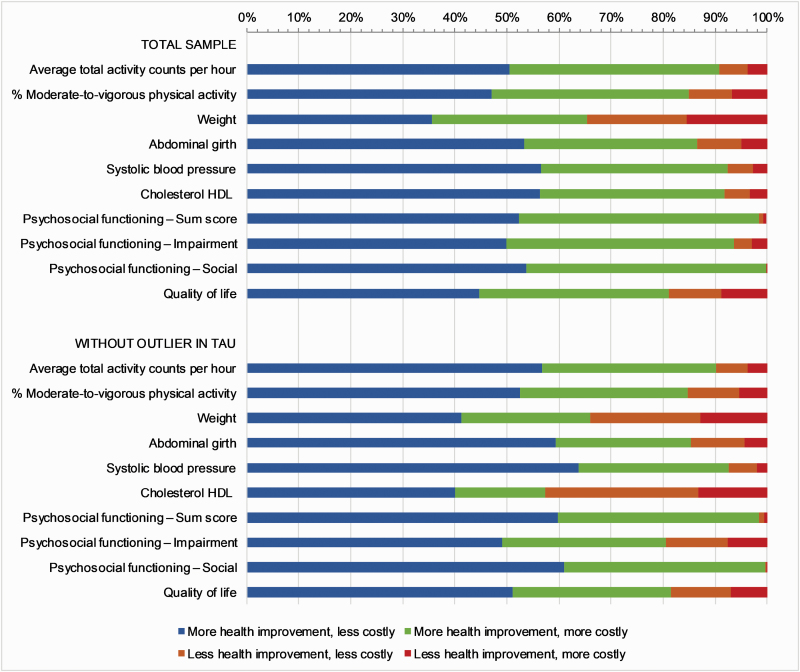
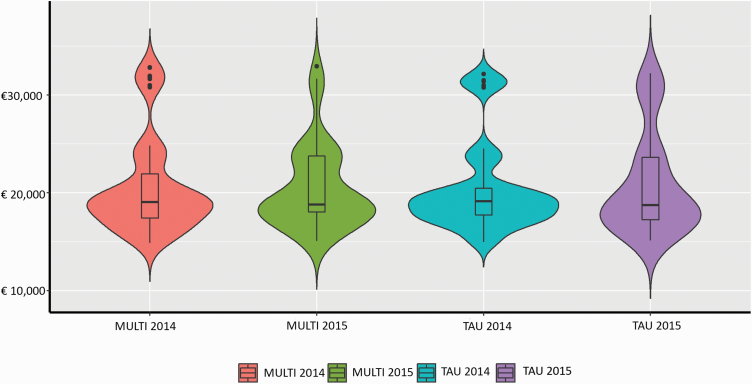
Economic evaluations of lifestyle interventions for people with mental illness are needed to inform policymakers and managers about implementing such interventions and corresponding reforms in routine mental healthcare. We aimed to evaluate changes in healthcare costs 18 months after the implementation of a multidisciplinary lifestyle-enhancing treatment for inpatients with severe mental illness (MULTI) versus treatment as usual (TAU). In a cohort study (n = 114; 65 MULTI, 49 TAU), we retrospectively retrieved cost data in Euros on all patient sessions, ward stay, medication use, and hospital referrals in the quarter year at the start of MULTI (Q1 2014) and after its evaluation (Q3 2015). We used linear regression analyses correcting for baseline values and differences between groups, calculated deterministic incremental cost-effectiveness ratios for previously shown changes in physical activity, metabolic health, psychosocial functioning, and additionally quality of life, and performed probabilistic sensitivity analyses including cost-effectiveness planes. Adjusted regression showed reduced total costs per patient per quarter year in favor of MULTI (B = -736.30, 95%CI: -2145.2 to 672.6). Corresponding probabilistic sensitivity analyses accounting for uncertainty surrounding the parameters showed statistically non-significant cost savings against health improvements for all health-related outcomes in MULTI compared to TAU. It is concluded that MULTI did not increase healthcare costs while improving health outcomes. This indicates that starting lifestyle interventions does not need to be hampered by costs. Potential societal and economic value may justify investment to support implementation and maintenance. Further research is needed to study this hypothesis.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
