{"title":"Survival and Disease Progression in Older Adult Patients With Cirrhosis: A Retrospective Study.","authors":"Khaled Al-Smadi, Ammar Qureshi, Michelle Buitrago, Besher Ashouri, Zeid Kayali","doi":"10.1155/2024/5852680","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Cirrhosis incidence in older adult patients has been increasing with limited data on their survival. This study is aimed at investigating the survival and disease progression in older adult patients with cirrhosis compared to younger patients. <b>Methods:</b> This is a retrospective single-center study. Patients aged above 50 with a confirmed diagnosis of cirrhosis based on biopsy, FibroSure test, splenomegaly, and low platelets < 120 × 10<sup>9</sup>/L) or imaging findings including FibroScan were included. Patients with active substance abuse, transjugular intrahepatic portosystemic shunt (TIPS), prior spontaneous bacterial peritonitis (SBP), variceal hemorrhage, model for end-stage liver disease-Na (MELD - Na) ≥ 20, had liver transplantation, malignancy except for squamous cell carcinoma, and other comorbidities such as congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), and end-stage kidney disease with glomerular filtration rate (GFR) < 30 were excluded. Patients' records from the liver clinic were reviewed and demographics, laboratory, and compensation and decompensation status were collated. Patients were separated into two groups based on age 50-64 years and age ≥ 65. The primary endpoint was death, and the secondary endpoint was disease progression measured by the baseline to 12-month increase in MELD-Na score. The Kaplan-Meier analysis was conducted to compare the survival between the two groups. Cox regression analysis was performed to identify independent risk factors for poor survival. <b>Results:</b> A total of 191 patients diagnosed with cirrhosis met the inclusion and exclusion criteria. There were 80 patients aged 50-64 years and 111 patients aged ≥ 65 years. Significantly shorter survival times were seen among patients aged ≥ 65 years compared to those aged 50-64 years (73.3 ± 4.8 vs. 151.5 ± 22.7; <i>p</i> < .001). Age of diagnosis ≥ 65 years (<i>p</i> < 0.001), male gender (<i>p</i> = .013), body mass index (BMI) < 30 (<i>p</i> = 0.005), and decompensation (<i>p</i> = 0.008) were found to be independent risk factors for poor survival. MELD-Na scores increased significantly in 12 months of follow-up from baseline, but only in patients with decompensated cirrhosis (<i>p</i> = 0.013). <b>Conclusions:</b> Cirrhotic patients aged ≥ 65 years have significantly poor survival compared to younger patients. A prospective study is needed to further investigate the effect of age and obesity on survival and disease progression in older adult patients with cirrhosis.</p>","PeriodicalId":46297,"journal":{"name":"International Journal of Hepatology","volume":"2024 ","pages":"5852680"},"PeriodicalIF":1.4000,"publicationDate":"2024-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11326880/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/5852680","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
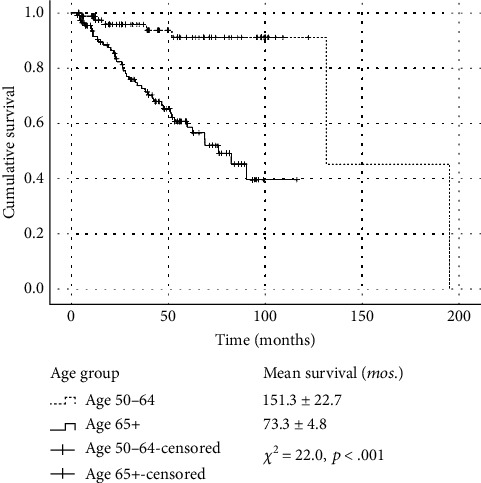
Background: Cirrhosis incidence in older adult patients has been increasing with limited data on their survival. This study is aimed at investigating the survival and disease progression in older adult patients with cirrhosis compared to younger patients. Methods: This is a retrospective single-center study. Patients aged above 50 with a confirmed diagnosis of cirrhosis based on biopsy, FibroSure test, splenomegaly, and low platelets < 120 × 109/L) or imaging findings including FibroScan were included. Patients with active substance abuse, transjugular intrahepatic portosystemic shunt (TIPS), prior spontaneous bacterial peritonitis (SBP), variceal hemorrhage, model for end-stage liver disease-Na (MELD - Na) ≥ 20, had liver transplantation, malignancy except for squamous cell carcinoma, and other comorbidities such as congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), and end-stage kidney disease with glomerular filtration rate (GFR) < 30 were excluded. Patients' records from the liver clinic were reviewed and demographics, laboratory, and compensation and decompensation status were collated. Patients were separated into two groups based on age 50-64 years and age ≥ 65. The primary endpoint was death, and the secondary endpoint was disease progression measured by the baseline to 12-month increase in MELD-Na score. The Kaplan-Meier analysis was conducted to compare the survival between the two groups. Cox regression analysis was performed to identify independent risk factors for poor survival. Results: A total of 191 patients diagnosed with cirrhosis met the inclusion and exclusion criteria. There were 80 patients aged 50-64 years and 111 patients aged ≥ 65 years. Significantly shorter survival times were seen among patients aged ≥ 65 years compared to those aged 50-64 years (73.3 ± 4.8 vs. 151.5 ± 22.7; p < .001). Age of diagnosis ≥ 65 years (p < 0.001), male gender (p = .013), body mass index (BMI) < 30 (p = 0.005), and decompensation (p = 0.008) were found to be independent risk factors for poor survival. MELD-Na scores increased significantly in 12 months of follow-up from baseline, but only in patients with decompensated cirrhosis (p = 0.013). Conclusions: Cirrhotic patients aged ≥ 65 years have significantly poor survival compared to younger patients. A prospective study is needed to further investigate the effect of age and obesity on survival and disease progression in older adult patients with cirrhosis.
期刊介绍:
International Journal of Hepatology is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies related to the medical, surgical, pathological, biochemical, and physiological aspects of hepatology, as well as the management of disorders affecting the liver, gallbladder, biliary tree, and pancreas.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
