Kajsa M.L. Fridström , René M. Winter , Natalie Hornik , Sigrun S. Almberg , Signe Danielsen , Kathrine R. Redalen
{"title":"Evaluation of magnetic resonance imaging derived synthetic computed tomography for proton therapy planning in prostate cancer","authors":"Kajsa M.L. Fridström , René M. Winter , Natalie Hornik , Sigrun S. Almberg , Signe Danielsen , Kathrine R. Redalen","doi":"10.1016/j.phro.2024.100625","DOIUrl":null,"url":null,"abstract":"<div><h3>Background and purpose</h3><p>Magnetic resonance imaging (MRI)-only workflow is used in photon radiotherapy (RT) today, but not yet for protons. To bring MRI-only proton RT into clinical use, proton dose calculation on MRI-derived synthetic CT (sCT) must be validated. We evaluated proton dose calculation accuracy of prostate cancer proton plans using a commercially available sCT generator already validated for photon planning.</p></div><div><h3>Materials and methods</h3><p>The retrospective planning study included 10 prostate cancer patients who underwent MRI and planning CT (pCT) before RT. sCT were generated from the MRI with MRI Planner v2.3, and compared to pCT using structural mean absolute error (MAE). The pCT was used to create one-arc volumetric modulated arc therapy (VMAT) photon plan and two-field intensity modulated proton therapy (IMPT) proton plan. Each plan was recalculated on the sCT and compared to pCT doses. Dose volume histogram parameters, gamma analyses and range differences were evaluated.</p></div><div><h3>Results</h3><p>Median MAE for the body contour was 71 HU. Dose differences between pCT and sCT were small and similar for VMAT and IMPT plans. Median (range) gamma pass rates were lower for IMPT plans with 95.8 (89.3–98.7) % compared to VMAT plans with 99.4 (91.2–99.6) %. The proton range difference was 1.0 (interquartile range –0.1 – 0.2) mm deeper for sCT compared to the reference.</p></div><div><h3>Conclusion</h3><p>MRI-only IMPT planning for prostate cancer seems feasible in a clinical setting for the evaluated beam arrangement and sCT generator. More patients and evaluation of other beam arrangements are needed for a more general conclusion.</p></div>","PeriodicalId":36850,"journal":{"name":"Physics and Imaging in Radiation Oncology","volume":"31 ","pages":"Article 100625"},"PeriodicalIF":3.3000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2405631624000952/pdfft?md5=bdff56b24bab3515231eb6ae2a486b75&pid=1-s2.0-S2405631624000952-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Physics and Imaging in Radiation Oncology","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2405631624000952","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/12 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and purpose
Magnetic resonance imaging (MRI)-only workflow is used in photon radiotherapy (RT) today, but not yet for protons. To bring MRI-only proton RT into clinical use, proton dose calculation on MRI-derived synthetic CT (sCT) must be validated. We evaluated proton dose calculation accuracy of prostate cancer proton plans using a commercially available sCT generator already validated for photon planning.
Materials and methods
The retrospective planning study included 10 prostate cancer patients who underwent MRI and planning CT (pCT) before RT. sCT were generated from the MRI with MRI Planner v2.3, and compared to pCT using structural mean absolute error (MAE). The pCT was used to create one-arc volumetric modulated arc therapy (VMAT) photon plan and two-field intensity modulated proton therapy (IMPT) proton plan. Each plan was recalculated on the sCT and compared to pCT doses. Dose volume histogram parameters, gamma analyses and range differences were evaluated.
Results
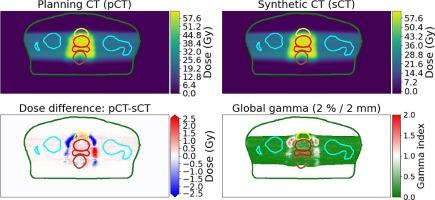
Median MAE for the body contour was 71 HU. Dose differences between pCT and sCT were small and similar for VMAT and IMPT plans. Median (range) gamma pass rates were lower for IMPT plans with 95.8 (89.3–98.7) % compared to VMAT plans with 99.4 (91.2–99.6) %. The proton range difference was 1.0 (interquartile range –0.1 – 0.2) mm deeper for sCT compared to the reference.
Conclusion
MRI-only IMPT planning for prostate cancer seems feasible in a clinical setting for the evaluated beam arrangement and sCT generator. More patients and evaluation of other beam arrangements are needed for a more general conclusion.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
