Alessandro Varrica, Mauro Cotza, Mauro Lo Rito, Angela Satriano, Giovanni Carboni, Antonio Saracino, Matteo Reali, Mahmood Hafdhullah, Marco Ranucci, Alessandro Giamberti
{"title":"Post cardiotomy extracorporeal membrane oxygenation in pediatric patients: Results and neurodevelopmental outcomes","authors":"Alessandro Varrica, Mauro Cotza, Mauro Lo Rito, Angela Satriano, Giovanni Carboni, Antonio Saracino, Matteo Reali, Mahmood Hafdhullah, Marco Ranucci, Alessandro Giamberti","doi":"10.1111/aor.14842","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>The increasing complexity of congenital cardiac surgery has led to greater utilization of extracorporeal membrane oxygenation (ECMO) support for children post-surgery. This study aims to identify risk factors for mortality and brain injury in pediatric patients requiring post-cardiotomy ECMO and to evaluate their neurological outcomes.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This retrospective study includes pediatric patients with congenital heart diseases who required ECMO after surgery. Risk factors for in-hospital mortality and brain injury were assessed. Neurodevelopmental status was determined using the Pediatric Cerebral Performance Category (PCPC) Scale at discharge and during follow-up.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Between October 2014 and May 2021, 2651 pediatric patients underwent cardiac surgery, with 90 (3.4%) requiring ECMO. The mean age was 0.6 years, ranging from 1 day to 13 years and 7 months. ECMO was implemented for 45 patients due to CPB weaning failure (NW-CPB), 24 due to postoperative low-cardiac output syndrome (LCOS), and 21 for extracorporeal cardiopulmonary resuscitation (E-CPR). ECMO weaning was achieved in 73 patients (81%), with an overall mortality rate of 36%. Pre-implant lactate levels (OR: 1.13, 95% CI: 1.03–1.25; <i>p</i> = 0.009) and peak bilirubin levels (OR: 1.04, 95% CI: 0.87–1.24; <i>p</i> = 0.69) were risk factors for in-hospital mortality. Survival rates were 79% for LCOS, 60% for NW-CPB, and 48% for E-CPR. Brain injury incidence was 33%, with E-CPR being a significant risk factor (<i>p</i> = 0.006) and NW-CPB being protective (<i>p</i> = 0.001). Follow-up in November 2023 showed significant improvement in neurodevelopmental status (<i>p</i> < 0.001).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Elevated pre-implant lactate and elevated bilirubin levels during ECMO are major risk factors for mortality. E-CPR is the primary risk factor for brain injury. Follow-up revealed significant improvements in neurodevelopmental outcomes.</p>\n </section>\n </div>","PeriodicalId":8450,"journal":{"name":"Artificial organs","volume":"48 12","pages":"1525-1535"},"PeriodicalIF":2.3000,"publicationDate":"2024-08-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/aor.14842","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Artificial organs","FirstCategoryId":"5","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/aor.14842","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENGINEERING, BIOMEDICAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background
The increasing complexity of congenital cardiac surgery has led to greater utilization of extracorporeal membrane oxygenation (ECMO) support for children post-surgery. This study aims to identify risk factors for mortality and brain injury in pediatric patients requiring post-cardiotomy ECMO and to evaluate their neurological outcomes.
Methods
This retrospective study includes pediatric patients with congenital heart diseases who required ECMO after surgery. Risk factors for in-hospital mortality and brain injury were assessed. Neurodevelopmental status was determined using the Pediatric Cerebral Performance Category (PCPC) Scale at discharge and during follow-up.
Results
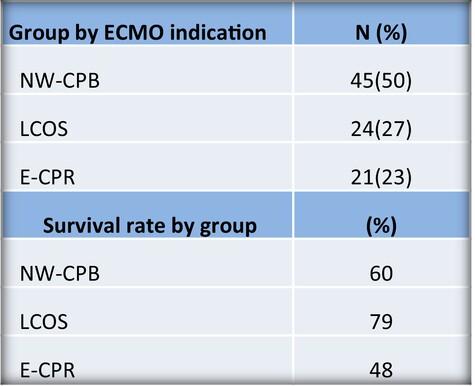
Between October 2014 and May 2021, 2651 pediatric patients underwent cardiac surgery, with 90 (3.4%) requiring ECMO. The mean age was 0.6 years, ranging from 1 day to 13 years and 7 months. ECMO was implemented for 45 patients due to CPB weaning failure (NW-CPB), 24 due to postoperative low-cardiac output syndrome (LCOS), and 21 for extracorporeal cardiopulmonary resuscitation (E-CPR). ECMO weaning was achieved in 73 patients (81%), with an overall mortality rate of 36%. Pre-implant lactate levels (OR: 1.13, 95% CI: 1.03–1.25; p = 0.009) and peak bilirubin levels (OR: 1.04, 95% CI: 0.87–1.24; p = 0.69) were risk factors for in-hospital mortality. Survival rates were 79% for LCOS, 60% for NW-CPB, and 48% for E-CPR. Brain injury incidence was 33%, with E-CPR being a significant risk factor (p = 0.006) and NW-CPB being protective (p = 0.001). Follow-up in November 2023 showed significant improvement in neurodevelopmental status (p < 0.001).
Conclusion
Elevated pre-implant lactate and elevated bilirubin levels during ECMO are major risk factors for mortality. E-CPR is the primary risk factor for brain injury. Follow-up revealed significant improvements in neurodevelopmental outcomes.
期刊介绍:
Artificial Organs is the official peer reviewed journal of The International Federation for Artificial Organs (Members of the Federation are: The American Society for Artificial Internal Organs, The European Society for Artificial Organs, and The Japanese Society for Artificial Organs), The International Faculty for Artificial Organs, the International Society for Rotary Blood Pumps, The International Society for Pediatric Mechanical Cardiopulmonary Support, and the Vienna International Workshop on Functional Electrical Stimulation. Artificial Organs publishes original research articles dealing with developments in artificial organs applications and treatment modalities and their clinical applications worldwide. Membership in the Societies listed above is not a prerequisite for publication. Articles are published without charge to the author except for color figures and excess page charges as noted.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
