{"title":"Model-Informed Approaches to Optimizing Therapeutics in the African Patient Populations","authors":"Mwila Mulubwa, Kelly Chibale","doi":"10.1002/cpt.3425","DOIUrl":null,"url":null,"abstract":"<p>Pharmacokinetics variability arises from individual differences in how drugs are absorbed, distributed, metabolized, and excreted by the body. Pharmacokinetic variations can be influenced by several intrinsic and extrinsic factors, including genetic polymorphisms, weight, sex, age, disease state, or polypharmacy.<span><sup>1</sup></span> Genetic factors such as polymorphisms in drug metabolizing enzymes can account for 20 to 95 percent patient variability in response to individual pharmacotherapy.<span><sup>1</sup></span></p><p>Understanding the genetic diversity in genes encoding for drug-metabolizing enzymes is essential in facilitating the development of more effective therapeutics tailored to diverse populations. Africa exhibits higher genetic diversity than other populations worldwide, a characteristic that extends to variability within genes encoding the cytochrome P450 enzyme system and drug transporter proteins.<span><sup>2</sup></span> It is noteworthy that genetic variability in African populations is not representative of that in the African American population and therefore cannot be assumed to be similar. Variations in gene sequence ultimately translate into decreased, normal, increased, or no enzyme function. This gives rise to metabolic phenotypes such as poor metabolizers, normal metabolizers, and fast metabolizers, which are associated with adverse drug reactions, suboptimal treatment efficacy, and poor treatment outcomes, respectively. This genetic variability has contributed to the high incidences of adverse drug reactions and poor therapeutic outcomes, especially in tuberculosis (TB) and human immunodeficiency virus (HIV) cases reported in Africa.<span><sup>2</sup></span> Hence, variations in pharmacokinetics pose challenges and create disparities in treatment outcomes among the genetically diverse African populations.</p><p>These challenges are compounded by lack of sufficiently powered clinical pharmacokinetics or pharmacogenetics studies to accurately quantify the influence of the prevalent pharmacogenetic variants on drug exposure in most African populations.<span><sup>3</sup></span> In addition, despite Africa accounting for around 15% of the global population, it remains understudied and largely absent from biomedical research. Therefore, it is indispensable to adopt model-informed strategies to address disparities in therapeutic outcomes among African patient populations. These approaches involve the application of data-driven models to guide decision-making and optimize therapeutic interventions for African patient populations. In the absence of African-derived biobanks, this requires the building or refining of existing physiologically based pharmacokinetic (PBPK) models that factor in African genetic variants predicted from artificial intelligence (AI) as illustrated in <b>Figure</b> 1. Here, we propose <i>in vitro</i> and <i>in silico</i> methods that may help explain pharmacokinetic variability and inform dose regimen optimization. By incorporating information such as genetic factors, comorbidities such as TB infection, and treatment response patterns, healthcare providers can tailor therapies to the specific needs of African patients.</p><p>Tuberculosis (TB) is a serious infectious disease that is caused by <i>Mycobacterium tuberculosis</i> (<i>Mtb</i>) and mostly affects not only the lungs but also other organs. Treatment typically involves a combination of antibiotics taken over a long period (4–6 months for drug sensitive TB and 6–20 months for drug-resistant TB) to eliminate the bacteria and prevent the development of drug-resistant strains. The burden of <i>Mtb</i> is high, particularly in low- and middle-income countries of Africa where co-morbidities are prevalent. The burden of noncommunicable diseases (NCDs) in Africa such as diabetes and cardiovascular diseases are a growing concern, accounting for over 30% of the continent's mortality. These NCDs also account for the most common comorbidities in tuberculosis patients. The impact of comorbid conditions on the PK of drugs used to treat <i>Mtb</i> is a crucial area of study, as these interactions can potentially affect treatment outcomes.<span><sup>4</sup></span> Understanding how comorbidities such as hypertension, diabetes and HIV infection can influence the PK is essential for optimizing therapeutic regimens. Given the high burden of <i>Mtb</i> coinfections worldwide, it is important to explore the complex interplay between the <i>Mtb</i> infection and other comorbidities to develop more effective treatment strategies.</p><p>Metabolism of drugs is mostly attributed to liver enzymes particularly the cytochrome P450s. <i>Mtb</i> possesses its own set of enzymes (<b>Table</b> 1) capable of catalyzing biotransformation reactions on xenobiotics, including some antituberculosis drugs. These enzymes enable <i>Mtb</i> to modulate the activity of drugs through various mechanisms, such as deactivation or activation of drugs, ultimately influencing the effectiveness of TB treatment.<span><sup>5, 6</sup></span> The extent of <i>Mtb</i> drug metabolism is dependent on the bacterial load. It was shown in a large cohort of African patients receiving first-line antituberculosis drugs (isoniazid, rifampicin, pyrazinamide, and ethambutol) that <i>Mtb</i> bacterial load persisted to an average amount of 2 log<sub>10</sub> CFU/mL after 12 weeks of treatment from an average baseline of 6 log<sub>10</sub> CFU/mL.<span><sup>7</sup></span> In the case of a drug that is metabolized by <i>Mtb</i>, it is expected for drug clearance to decrease or normalize after a longer duration of treatment. Hence, <i>Mtb</i>-mediated drug metabolism may potentially impact the efficacy and treatment outcomes of tuberculosis or other comorbidities whose drug treatment may be prone to <i>Mtb</i>-mediated metabolism.</p><p>Designing optimum treatment regimens using nonlinear-mixed effects (NLME) modeling and simulation represents an advanced approach to treatment optimization. The NLME modeling approach allows for the incorporation and modeling of <i>Mtb</i>-mediated metabolism or genetic factors as covariates into these mathematical models, enabling the exploration of complex pharmacokinetic scenarios. By leveraging pharmacokinetic data predicted from PBPK models, NLME modeling can characterize the variability in drug exposure and identify factors such as genetic factors, demographics, and disease status such as TB as significant covariates that influence treatment outcomes. Simulation techniques based on NLME models enable the exploration of different dosing strategies, treatment durations, and combination therapies <i>in silico</i>,<span><sup>10</sup></span> providing valuable insights into the optimal design of treatment regimens for specific African patient populations.</p><p>Improving therapeutic outcomes entails administration of the right dose or dose regimen. Model-informed approaches offer a promising avenue for optimizing therapeutics in the African patient population. By building PBPK models using African liver subcellular fractions or AI-predicted prevalent African gene variants (drug metabolizing enzymes) and integrating <i>Mtb</i>-mediated drug metabolism into PBPK models we can predict and capture pharmacokinetic variability. The NLME modeling of PBPK simulated pharmacokinetic profiles enhance the understanding of pharmacogenetic variability, which enables the development of more tailored and precise treatment regimens, minimizing the risk of adverse drug reactions and optimizing therapeutic outcomes among African populations.</p><p>K.C. is the Neville Isdell Chair in African-centric Drug Discovery and Development and thanks Neville Isdell for generously funding the Chair.</p><p>The authors declared no competing interests for this work.</p>","PeriodicalId":153,"journal":{"name":"Clinical Pharmacology & Therapeutics","volume":"116 6","pages":"1391-1394"},"PeriodicalIF":5.5000,"publicationDate":"2024-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cpt.3425","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacology & Therapeutics","FirstCategoryId":"3","ListUrlMain":"https://ascpt.onlinelibrary.wiley.com/doi/10.1002/cpt.3425","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Pharmacokinetics variability arises from individual differences in how drugs are absorbed, distributed, metabolized, and excreted by the body. Pharmacokinetic variations can be influenced by several intrinsic and extrinsic factors, including genetic polymorphisms, weight, sex, age, disease state, or polypharmacy.1 Genetic factors such as polymorphisms in drug metabolizing enzymes can account for 20 to 95 percent patient variability in response to individual pharmacotherapy.1
Understanding the genetic diversity in genes encoding for drug-metabolizing enzymes is essential in facilitating the development of more effective therapeutics tailored to diverse populations. Africa exhibits higher genetic diversity than other populations worldwide, a characteristic that extends to variability within genes encoding the cytochrome P450 enzyme system and drug transporter proteins.2 It is noteworthy that genetic variability in African populations is not representative of that in the African American population and therefore cannot be assumed to be similar. Variations in gene sequence ultimately translate into decreased, normal, increased, or no enzyme function. This gives rise to metabolic phenotypes such as poor metabolizers, normal metabolizers, and fast metabolizers, which are associated with adverse drug reactions, suboptimal treatment efficacy, and poor treatment outcomes, respectively. This genetic variability has contributed to the high incidences of adverse drug reactions and poor therapeutic outcomes, especially in tuberculosis (TB) and human immunodeficiency virus (HIV) cases reported in Africa.2 Hence, variations in pharmacokinetics pose challenges and create disparities in treatment outcomes among the genetically diverse African populations.
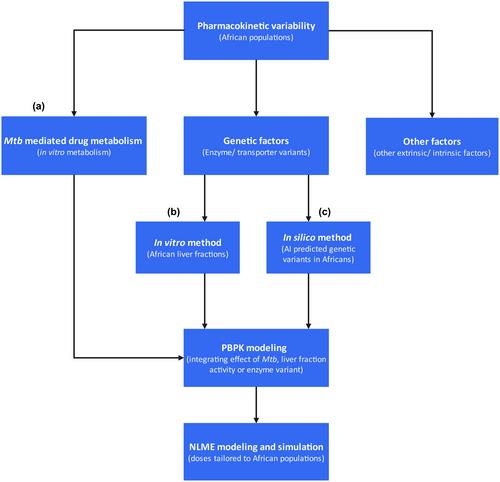
These challenges are compounded by lack of sufficiently powered clinical pharmacokinetics or pharmacogenetics studies to accurately quantify the influence of the prevalent pharmacogenetic variants on drug exposure in most African populations.3 In addition, despite Africa accounting for around 15% of the global population, it remains understudied and largely absent from biomedical research. Therefore, it is indispensable to adopt model-informed strategies to address disparities in therapeutic outcomes among African patient populations. These approaches involve the application of data-driven models to guide decision-making and optimize therapeutic interventions for African patient populations. In the absence of African-derived biobanks, this requires the building or refining of existing physiologically based pharmacokinetic (PBPK) models that factor in African genetic variants predicted from artificial intelligence (AI) as illustrated in Figure 1. Here, we propose in vitro and in silico methods that may help explain pharmacokinetic variability and inform dose regimen optimization. By incorporating information such as genetic factors, comorbidities such as TB infection, and treatment response patterns, healthcare providers can tailor therapies to the specific needs of African patients.
Tuberculosis (TB) is a serious infectious disease that is caused by Mycobacterium tuberculosis (Mtb) and mostly affects not only the lungs but also other organs. Treatment typically involves a combination of antibiotics taken over a long period (4–6 months for drug sensitive TB and 6–20 months for drug-resistant TB) to eliminate the bacteria and prevent the development of drug-resistant strains. The burden of Mtb is high, particularly in low- and middle-income countries of Africa where co-morbidities are prevalent. The burden of noncommunicable diseases (NCDs) in Africa such as diabetes and cardiovascular diseases are a growing concern, accounting for over 30% of the continent's mortality. These NCDs also account for the most common comorbidities in tuberculosis patients. The impact of comorbid conditions on the PK of drugs used to treat Mtb is a crucial area of study, as these interactions can potentially affect treatment outcomes.4 Understanding how comorbidities such as hypertension, diabetes and HIV infection can influence the PK is essential for optimizing therapeutic regimens. Given the high burden of Mtb coinfections worldwide, it is important to explore the complex interplay between the Mtb infection and other comorbidities to develop more effective treatment strategies.
Metabolism of drugs is mostly attributed to liver enzymes particularly the cytochrome P450s. Mtb possesses its own set of enzymes (Table 1) capable of catalyzing biotransformation reactions on xenobiotics, including some antituberculosis drugs. These enzymes enable Mtb to modulate the activity of drugs through various mechanisms, such as deactivation or activation of drugs, ultimately influencing the effectiveness of TB treatment.5, 6 The extent of Mtb drug metabolism is dependent on the bacterial load. It was shown in a large cohort of African patients receiving first-line antituberculosis drugs (isoniazid, rifampicin, pyrazinamide, and ethambutol) that Mtb bacterial load persisted to an average amount of 2 log10 CFU/mL after 12 weeks of treatment from an average baseline of 6 log10 CFU/mL.7 In the case of a drug that is metabolized by Mtb, it is expected for drug clearance to decrease or normalize after a longer duration of treatment. Hence, Mtb-mediated drug metabolism may potentially impact the efficacy and treatment outcomes of tuberculosis or other comorbidities whose drug treatment may be prone to Mtb-mediated metabolism.
Designing optimum treatment regimens using nonlinear-mixed effects (NLME) modeling and simulation represents an advanced approach to treatment optimization. The NLME modeling approach allows for the incorporation and modeling of Mtb-mediated metabolism or genetic factors as covariates into these mathematical models, enabling the exploration of complex pharmacokinetic scenarios. By leveraging pharmacokinetic data predicted from PBPK models, NLME modeling can characterize the variability in drug exposure and identify factors such as genetic factors, demographics, and disease status such as TB as significant covariates that influence treatment outcomes. Simulation techniques based on NLME models enable the exploration of different dosing strategies, treatment durations, and combination therapies in silico,10 providing valuable insights into the optimal design of treatment regimens for specific African patient populations.
Improving therapeutic outcomes entails administration of the right dose or dose regimen. Model-informed approaches offer a promising avenue for optimizing therapeutics in the African patient population. By building PBPK models using African liver subcellular fractions or AI-predicted prevalent African gene variants (drug metabolizing enzymes) and integrating Mtb-mediated drug metabolism into PBPK models we can predict and capture pharmacokinetic variability. The NLME modeling of PBPK simulated pharmacokinetic profiles enhance the understanding of pharmacogenetic variability, which enables the development of more tailored and precise treatment regimens, minimizing the risk of adverse drug reactions and optimizing therapeutic outcomes among African populations.
K.C. is the Neville Isdell Chair in African-centric Drug Discovery and Development and thanks Neville Isdell for generously funding the Chair.
The authors declared no competing interests for this work.
期刊介绍:
Clinical Pharmacology & Therapeutics (CPT) is the authoritative cross-disciplinary journal in experimental and clinical medicine devoted to publishing advances in the nature, action, efficacy, and evaluation of therapeutics. CPT welcomes original Articles in the emerging areas of translational, predictive and personalized medicine; new therapeutic modalities including gene and cell therapies; pharmacogenomics, proteomics and metabolomics; bioinformation and applied systems biology complementing areas of pharmacokinetics and pharmacodynamics, human investigation and clinical trials, pharmacovigilence, pharmacoepidemiology, pharmacometrics, and population pharmacology.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
