Association between new insertion of a long-term enteral feeding tube and mortality in adults admitted to the hospital with aspiration: A retrospective cohort study
Anthony D. Bai MD, MSc, Siddhartha Srivastava MD, MSc, Marie Leung MD, Heather Johnson MD, Amol A. Verma MD, MPhil, Fahad Razak MD, MSc
{"title":"Association between new insertion of a long-term enteral feeding tube and mortality in adults admitted to the hospital with aspiration: A retrospective cohort study","authors":"Anthony D. Bai MD, MSc, Siddhartha Srivastava MD, MSc, Marie Leung MD, Heather Johnson MD, Amol A. Verma MD, MPhil, Fahad Razak MD, MSc","doi":"10.1002/jpen.2680","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>We aimed to describe the association between insertion of a new long-term enteral feeding tube during admission for aspiration and in-hospital mortality.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This retrospective cohort study across 28 Canadian hospitals from 2015 to 2022 included consecutive patients who were admitted for aspiration. Patients were categorized based on new long-term enteral feeding tube insertion during hospital stay or not. The primary outcome was the time to death in hospital. Secondary outcomes included time to discharge alive and hospital readmission for aspiration within 90 days. We used propensity score weighting to balance covariates, and a competing risk model to describe in-hospital death and discharge.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Of 12,850 patients admitted for aspiration, 852 (6.6%) patients received a long-term enteral feeding tube. In the hospital, 184 (21.6%) and 2489 (20.8%) patients in the enteral feeding tube group and no enteral feeding tube group died, respectively. Within 90 days of discharge, 127 (14.9%) and 1148 (9.6%) patients in the enteral feeding tube and no enteral feeding tube group were readmitted for aspiration, respectively. After balancing covariates, an enteral feeding tube was associated with a similar in-hospital mortality risk (subdistribution hazard ratio [sHR] = 1.05, 95% CI = 0.89–1.23; <i>P</i> = 0.5800), longer time to discharge alive (sHR = 0.58, 95% CI = 0.54–0.63; <i>P</i> < 0.0001), and a higher risk of readmission (risk difference = 5.0%, 95% CI = 2.4%–7.6%; <i>P</i> = 0.0001).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Initiation of long-term enteral tube feeding was not uncommon after admission for aspiration and was not associated with an improvement in the probability of being discharged alive from the hospital or readmitted for aspiration.</p>\n </section>\n </div>","PeriodicalId":16668,"journal":{"name":"Journal of Parenteral and Enteral Nutrition","volume":"48 7","pages":"841-849"},"PeriodicalIF":4.1000,"publicationDate":"2024-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jpen.2680","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Parenteral and Enteral Nutrition","FirstCategoryId":"3","ListUrlMain":"https://aspenjournals.onlinelibrary.wiley.com/doi/10.1002/jpen.2680","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"NUTRITION & DIETETICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
We aimed to describe the association between insertion of a new long-term enteral feeding tube during admission for aspiration and in-hospital mortality.
Methods
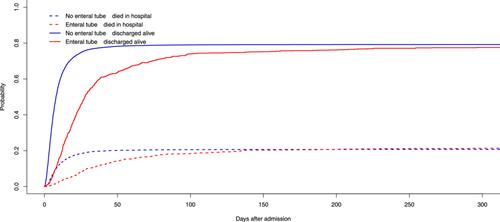
This retrospective cohort study across 28 Canadian hospitals from 2015 to 2022 included consecutive patients who were admitted for aspiration. Patients were categorized based on new long-term enteral feeding tube insertion during hospital stay or not. The primary outcome was the time to death in hospital. Secondary outcomes included time to discharge alive and hospital readmission for aspiration within 90 days. We used propensity score weighting to balance covariates, and a competing risk model to describe in-hospital death and discharge.
Results
Of 12,850 patients admitted for aspiration, 852 (6.6%) patients received a long-term enteral feeding tube. In the hospital, 184 (21.6%) and 2489 (20.8%) patients in the enteral feeding tube group and no enteral feeding tube group died, respectively. Within 90 days of discharge, 127 (14.9%) and 1148 (9.6%) patients in the enteral feeding tube and no enteral feeding tube group were readmitted for aspiration, respectively. After balancing covariates, an enteral feeding tube was associated with a similar in-hospital mortality risk (subdistribution hazard ratio [sHR] = 1.05, 95% CI = 0.89–1.23; P = 0.5800), longer time to discharge alive (sHR = 0.58, 95% CI = 0.54–0.63; P < 0.0001), and a higher risk of readmission (risk difference = 5.0%, 95% CI = 2.4%–7.6%; P = 0.0001).
Conclusion
Initiation of long-term enteral tube feeding was not uncommon after admission for aspiration and was not associated with an improvement in the probability of being discharged alive from the hospital or readmitted for aspiration.
期刊介绍:
The Journal of Parenteral and Enteral Nutrition (JPEN) is the premier scientific journal of nutrition and metabolic support. It publishes original peer-reviewed studies that define the cutting edge of basic and clinical research in the field. It explores the science of optimizing the care of patients receiving enteral or IV therapies. Also included: reviews, techniques, brief reports, case reports, and abstracts.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
