{"title":"Importance of ECG findings in COVID-19 patients: Predictor of in-hospital prognosis.","authors":"Mahsa Behnemoon, Mojhdeh Mehrno, Vahid Alinejad","doi":"10.48305/arya.2023.41600.2887","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiac injury in COVID-19 patients confers a worse prognosis. The interpretation of electrocardiography can be beneficial in the early diagnosis of probable cardiac involvement. After adjusting for other variables, we sought to determine if the initial ECG on admission could add additional prognostic value.</p><p><strong>Methods: </strong>In this single-center cross-sectional study, 1165 patients with a positive COVID-19 PCR between Feb 2020 and Nov 2021 were enrolled in our study. Patients were grouped according to their admitted units, and survivors to hospital discharge or non-survivors. Predictors of ICU admission and in-hospital mortality were determined using univariate analysis and a logistic regression model.</p><p><strong>Results: </strong>The mean age was 55.6 ± 16.2 years and 52% were male. Out of 1165 patients, 149 deaths (12.8%) were recorded during hospitalization. Sinus tachycardia was the most common dysrhythmia, followed by premature atrial and ventricular beats, sinus bradycardia, and atrial fibrillation (28.6%, 5.6%, 3.9%, and 2.1%, respectively). Age (p<0.001), sex (p=0.006), history of diabetes mellitus (p=0.002), hypertension (p=0.018), ischemic heart disease (p=0.004), and cancer (p<0.001) were more frequent among non-survivors. Among ECG findings, tachycardia, low voltage QRS, ST-T changes, and dysrhythmia were related to an increased mortality risk. However, in regression analysis, only sex (OR 1.89, 95% CI 1.2 to 2.9, p=0.004), age (OR 1.03, 95% CI 1.02 to 1.05, p<0.001), and initial tachycardia (OR 1.02, 95% CI 1.01 to 1.03, p<0.001) were independent predictors of in-hospital mortality.</p><p><strong>Conclusion: </strong>Our data suggest that initial electrocardiographic findings could be helpful in distinguishing patients with an increased risk for ICU admission or in-hospital death.</p>","PeriodicalId":46477,"journal":{"name":"ARYA Atherosclerosis","volume":"20 1","pages":"41-50"},"PeriodicalIF":0.6000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11331551/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ARYA Atherosclerosis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.48305/arya.2023.41600.2887","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cardiac injury in COVID-19 patients confers a worse prognosis. The interpretation of electrocardiography can be beneficial in the early diagnosis of probable cardiac involvement. After adjusting for other variables, we sought to determine if the initial ECG on admission could add additional prognostic value.
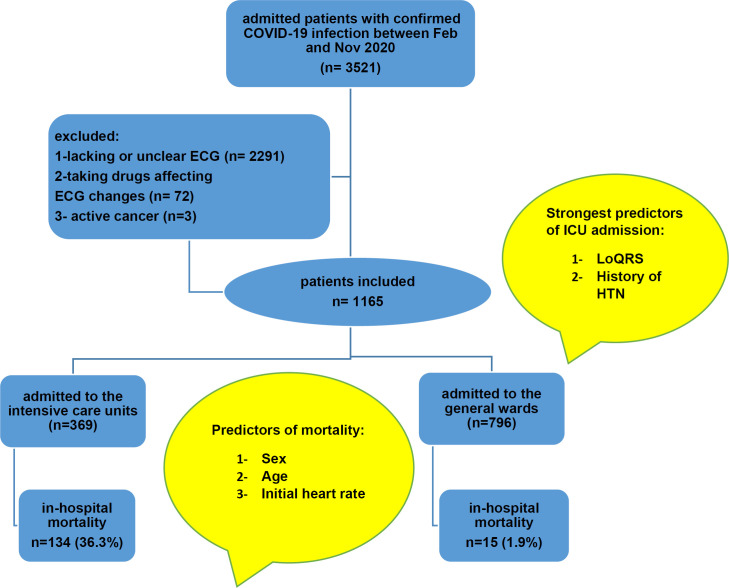
Methods: In this single-center cross-sectional study, 1165 patients with a positive COVID-19 PCR between Feb 2020 and Nov 2021 were enrolled in our study. Patients were grouped according to their admitted units, and survivors to hospital discharge or non-survivors. Predictors of ICU admission and in-hospital mortality were determined using univariate analysis and a logistic regression model.
Results: The mean age was 55.6 ± 16.2 years and 52% were male. Out of 1165 patients, 149 deaths (12.8%) were recorded during hospitalization. Sinus tachycardia was the most common dysrhythmia, followed by premature atrial and ventricular beats, sinus bradycardia, and atrial fibrillation (28.6%, 5.6%, 3.9%, and 2.1%, respectively). Age (p<0.001), sex (p=0.006), history of diabetes mellitus (p=0.002), hypertension (p=0.018), ischemic heart disease (p=0.004), and cancer (p<0.001) were more frequent among non-survivors. Among ECG findings, tachycardia, low voltage QRS, ST-T changes, and dysrhythmia were related to an increased mortality risk. However, in regression analysis, only sex (OR 1.89, 95% CI 1.2 to 2.9, p=0.004), age (OR 1.03, 95% CI 1.02 to 1.05, p<0.001), and initial tachycardia (OR 1.02, 95% CI 1.01 to 1.03, p<0.001) were independent predictors of in-hospital mortality.
Conclusion: Our data suggest that initial electrocardiographic findings could be helpful in distinguishing patients with an increased risk for ICU admission or in-hospital death.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
