Svenja F B J Mennens, Ellen Van der Spek, Janneke Ruinemans-Koerts, Marcel M G J Van Borren
{"title":"Hematologists/Physicians Need to Be Aware of Pseudohypercalcemia in Monoclonal Gammopathy: Lessons from a Case Report.","authors":"Svenja F B J Mennens, Ellen Van der Spek, Janneke Ruinemans-Koerts, Marcel M G J Van Borren","doi":"10.1155/2024/8844335","DOIUrl":null,"url":null,"abstract":"<p><p>We present a patient at risk of misdiagnosis with multiple myeloma due to pseudohypercalcemia. Examinations showed monoclonal protein, 50% monoclonal plasma cells in bone marrow, and hypercalcemia but no osteolytic bone lesions. Follow-up tests revealed pseudohypercalcemia, with elevated total calcium, but normal ionized calcium: a discrepancy due to calcium binding to monoclonal paraprotein (confirmed by laboratory experiments). Accordingly, the patient was diagnosed with smouldering myeloma. After 900 days, the presence of bone lesions prompted the start of treatment for myeloma. Consequently, monoclonal paraprotein levels declined and pseudohypercalcemia dissolved. Hence, ionized calcium should be measured in monoclonal gammopathies to avoid misdiagnosis.</p>","PeriodicalId":46307,"journal":{"name":"Case Reports in Hematology","volume":"2024 ","pages":"8844335"},"PeriodicalIF":0.7000,"publicationDate":"2024-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11347025/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/8844335","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
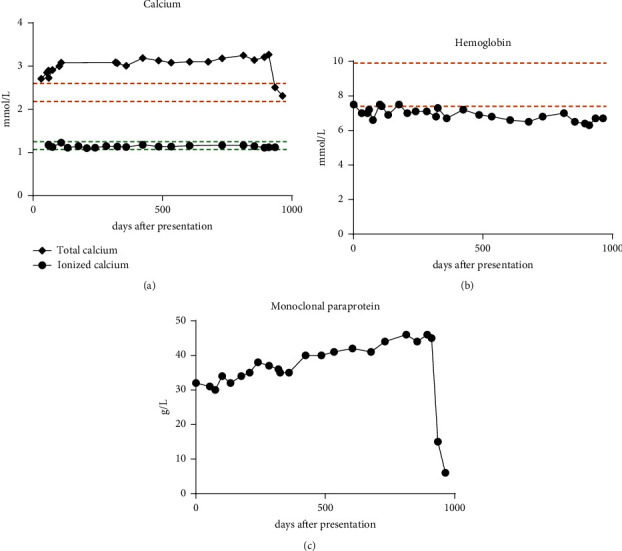
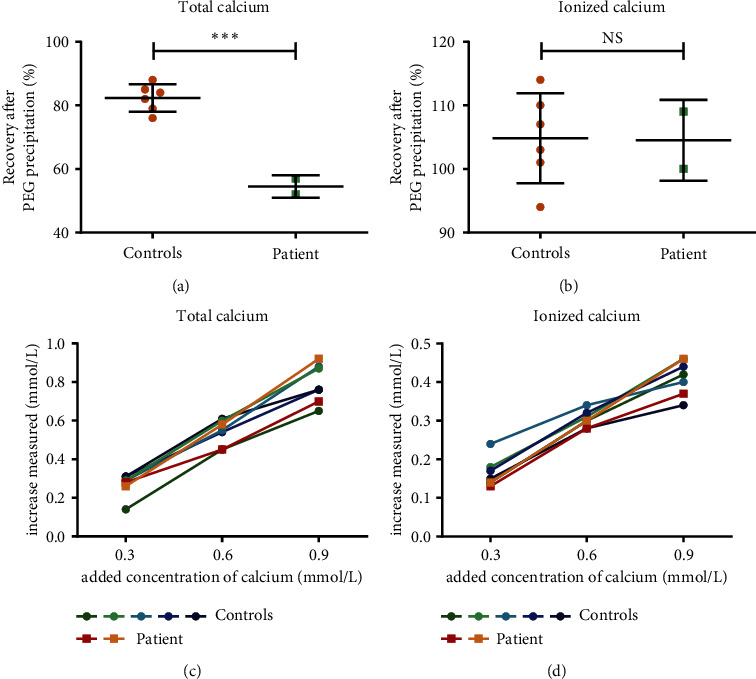
We present a patient at risk of misdiagnosis with multiple myeloma due to pseudohypercalcemia. Examinations showed monoclonal protein, 50% monoclonal plasma cells in bone marrow, and hypercalcemia but no osteolytic bone lesions. Follow-up tests revealed pseudohypercalcemia, with elevated total calcium, but normal ionized calcium: a discrepancy due to calcium binding to monoclonal paraprotein (confirmed by laboratory experiments). Accordingly, the patient was diagnosed with smouldering myeloma. After 900 days, the presence of bone lesions prompted the start of treatment for myeloma. Consequently, monoclonal paraprotein levels declined and pseudohypercalcemia dissolved. Hence, ionized calcium should be measured in monoclonal gammopathies to avoid misdiagnosis.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
