{"title":"Left Atrial Strain to Predict Postoperative Atrial Fibrillation in Patients Undergoing Off-pump Coronary Artery Bypass Graft","authors":"Deepak Prakash Borde MD, DNB, FCA, FTEE , Shreedhar Joshi MD, FCA, DM, FTEE , Ashish Agrawal DNB (Surg), MCh , Deepak Bhavsar MS, MCh , Pooja Joshi MD, FIACTA, FTEE , Pramod Apsingkar MD, DPM","doi":"10.1053/j.jvca.2024.07.047","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><div>Postoperative atrial fibrillation (POAF) is associated with increased morbidity, mortality, and length of hospital stay. The objective of this study was to assess the utility of left atrial strain (LAS) to predict POAF in patients undergoing off-pump coronary artery bypass grafting (OPCABG).</div></div><div><h3>Design</h3><div>Retrospective observational study.</div></div><div><h3>Setting</h3><div>Tertiary care hospital.</div></div><div><h3>Participants</h3><div>103 patients undergoing OPCABG.</div></div><div><h3>Interventions</h3><div>None.</div></div><div><h3>Measurements and Results</h3><div>In addition to comprehensive transthoracic echocardiography, LAS was measured for reservoir (R), conduction (CD), and contraction (CT) components. POAF was defined as new electrocardiographic evidence of AF requiring treatment. Logistic regression was done to assess factors associated with POAF. The diagnostic accuracy of variables in predicting POAF was assessed by receiver operating characteristic analysis. POAF was documented in 24 (23.3%) patients. There was no difference in ejection fraction, average global longitudinal strain, or proportion of left ventricular diastolic dysfunction grades between patients with POAF and patients without POAF. All three components of LAS: LAS R (19.2 ± 4.7 <em>v</em> 23.5 ± 4.8, p < 0.001), LAS CD (8.9 ± 3.7 <em>v</em> 12.3 ± 4.8, p = 0.1), and LAS CT (10.3 ± 3.9 <em>v</em> 12.1 ± 4.1, p = 0.04), were significantly lower among patients with POAF compared with patients without POAF, respectively. According to univariate analysis, all components of LAS were statistically significant predictors of POAF. In multivariate analysis, only age (odds ratio = 1.08, p = 0.025) and LAS R (odds ratio = 0.84, p = 0.004) were independently associated with POAF. LAS R was a better predictor of POAF, with an area under the curve (AUC) of 0.758, than LAS CD (AUC = 0.67) and LAS CT (AUC = 0.62). LAS R had an optimal cutoff of 23% with sensitivity of 95.8% (confidence interval: 78.9-99.9%) and specificity of 49.4% (37.9-60.9%) to predict POAF.</div></div><div><h3>Conclusions</h3><div>LAS R is a significant predictor of POAF, and its use can be recommended for screening of OPCABG patients at high risk of POAF.</div></div>","PeriodicalId":15176,"journal":{"name":"Journal of cardiothoracic and vascular anesthesia","volume":"38 11","pages":"Pages 2582-2591"},"PeriodicalIF":2.1000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cardiothoracic and vascular anesthesia","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1053077024005081","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/14 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
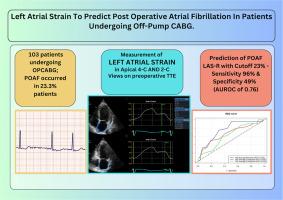
Postoperative atrial fibrillation (POAF) is associated with increased morbidity, mortality, and length of hospital stay. The objective of this study was to assess the utility of left atrial strain (LAS) to predict POAF in patients undergoing off-pump coronary artery bypass grafting (OPCABG).
Design
Retrospective observational study.
Setting
Tertiary care hospital.
Participants
103 patients undergoing OPCABG.
Interventions
None.
Measurements and Results
In addition to comprehensive transthoracic echocardiography, LAS was measured for reservoir (R), conduction (CD), and contraction (CT) components. POAF was defined as new electrocardiographic evidence of AF requiring treatment. Logistic regression was done to assess factors associated with POAF. The diagnostic accuracy of variables in predicting POAF was assessed by receiver operating characteristic analysis. POAF was documented in 24 (23.3%) patients. There was no difference in ejection fraction, average global longitudinal strain, or proportion of left ventricular diastolic dysfunction grades between patients with POAF and patients without POAF. All three components of LAS: LAS R (19.2 ± 4.7 v 23.5 ± 4.8, p < 0.001), LAS CD (8.9 ± 3.7 v 12.3 ± 4.8, p = 0.1), and LAS CT (10.3 ± 3.9 v 12.1 ± 4.1, p = 0.04), were significantly lower among patients with POAF compared with patients without POAF, respectively. According to univariate analysis, all components of LAS were statistically significant predictors of POAF. In multivariate analysis, only age (odds ratio = 1.08, p = 0.025) and LAS R (odds ratio = 0.84, p = 0.004) were independently associated with POAF. LAS R was a better predictor of POAF, with an area under the curve (AUC) of 0.758, than LAS CD (AUC = 0.67) and LAS CT (AUC = 0.62). LAS R had an optimal cutoff of 23% with sensitivity of 95.8% (confidence interval: 78.9-99.9%) and specificity of 49.4% (37.9-60.9%) to predict POAF.
Conclusions
LAS R is a significant predictor of POAF, and its use can be recommended for screening of OPCABG patients at high risk of POAF.
期刊介绍:
The Journal of Cardiothoracic and Vascular Anesthesia is primarily aimed at anesthesiologists who deal with patients undergoing cardiac, thoracic or vascular surgical procedures. JCVA features a multidisciplinary approach, with contributions from cardiac, vascular and thoracic surgeons, cardiologists, and other related specialists. Emphasis is placed on rapid publication of clinically relevant material.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
