{"title":"Endoscopic Resection of Stage T1 Colorectal Adenocarcinoma Followed by Surgical Intervention: a Single-center Retrospective Study.","authors":"Dongdong Zhang, Lin Chen, Jixiang Wu","doi":"10.1007/s12029-024-01109-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Domestic and international guidelines recommend endoscopic resection for stage T1 colorectal adenocarcinoma with indications. However, completion surgery remains imperative for patients exhibiting high-risk factors subsequent to endoscopic procedures.</p><p><strong>Objective: </strong>To investigate the evidence, pathological features, and surgical outcomes of completion surgery in patients with T1 colorectal adenocarcinoma following endoscopic resection.</p><p><strong>Methods: </strong>We retrospectively collect data on the clinical features and treatment outcomes of patients with stage T1 colorectal adenocarcinoma who underwent endoscopic resection followed by surgical resection and those who initially completed surgical intervention at Peking University International Hospital between January 2019 and October 2022, with the aim of assessing the necessity and feasibility of surgical intervention.</p><p><strong>Results: </strong>Seventeen patients (Group A) with high-risk factors following endoscopic procedure, especially with deep submucosal invasion and vascular or lymphatic invasion, experienced further surgical resection. The median interval between endoscopic resection and completion surgery was 23.71 days ± 15.89. Sixteen patients (Group B) underwent radical resection without any prior interventions. The surgical approach involves integration of laparoscopy and colonoscopy for precise localization and quantitative diagnosis, followed by radical surgery. The two groups demonstrated significant differences statistically with reference to tumor diameter (1.65 cm ± 0.77 vs 3.36 cm ± 1.39, P = 0.000) and the attainment of standard lymph node count (cases of detected lymph nodes larger than or equal to 12, 5 vs 12, P = 0.015). Postoperative complications and hospital stay manifested no significant disparity statistically in two groups. Patients who underwent completion surgery had no inferior outcomes compared with those who underwent direct surgery in terms of 5-year disease-free survival (Log rank test: P = 0.083, Breslow test: P = 0.089). The two groups also exhibited no significant differences statistically in the context of overall survival (Log rank test: P = 0.652, Breslow test: P = 0.758).</p><p><strong>Conclusion: </strong>Completion surgery is a safe and feasible treatment option for T1 colorectal adenocarcinoma patients with high-risk factors, particularly those with deep submucosal invasion and vascular or lymphatic invasion following endoscopic treatment. Furthermore, subsequent treatment should be chosen based on a comprehensive analysis of the patient's history of abdominal surgery, willingness, and pathological features.</p>","PeriodicalId":15895,"journal":{"name":"Journal of Gastrointestinal Cancer","volume":" ","pages":"1598-1606"},"PeriodicalIF":1.6000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11464598/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Gastrointestinal Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s12029-024-01109-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/31 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Domestic and international guidelines recommend endoscopic resection for stage T1 colorectal adenocarcinoma with indications. However, completion surgery remains imperative for patients exhibiting high-risk factors subsequent to endoscopic procedures.
Objective: To investigate the evidence, pathological features, and surgical outcomes of completion surgery in patients with T1 colorectal adenocarcinoma following endoscopic resection.
Methods: We retrospectively collect data on the clinical features and treatment outcomes of patients with stage T1 colorectal adenocarcinoma who underwent endoscopic resection followed by surgical resection and those who initially completed surgical intervention at Peking University International Hospital between January 2019 and October 2022, with the aim of assessing the necessity and feasibility of surgical intervention.
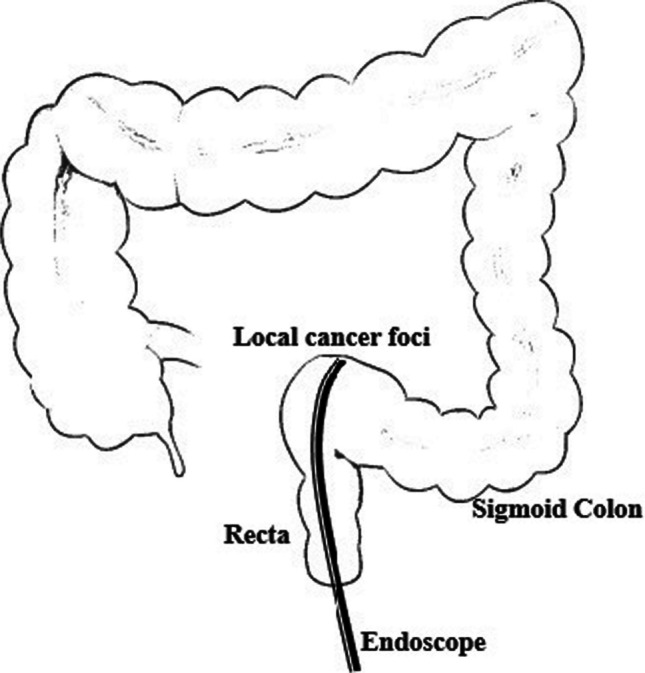
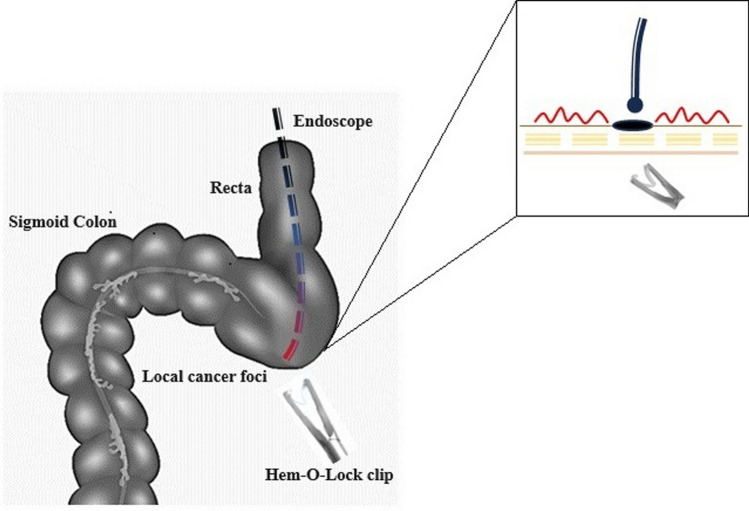
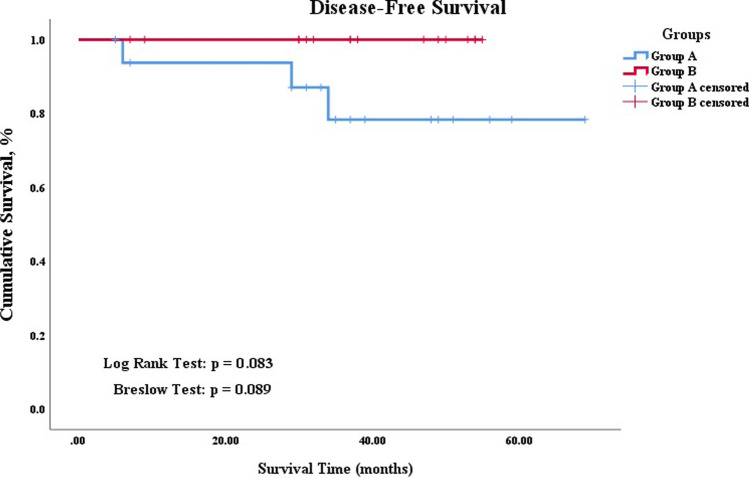
Results: Seventeen patients (Group A) with high-risk factors following endoscopic procedure, especially with deep submucosal invasion and vascular or lymphatic invasion, experienced further surgical resection. The median interval between endoscopic resection and completion surgery was 23.71 days ± 15.89. Sixteen patients (Group B) underwent radical resection without any prior interventions. The surgical approach involves integration of laparoscopy and colonoscopy for precise localization and quantitative diagnosis, followed by radical surgery. The two groups demonstrated significant differences statistically with reference to tumor diameter (1.65 cm ± 0.77 vs 3.36 cm ± 1.39, P = 0.000) and the attainment of standard lymph node count (cases of detected lymph nodes larger than or equal to 12, 5 vs 12, P = 0.015). Postoperative complications and hospital stay manifested no significant disparity statistically in two groups. Patients who underwent completion surgery had no inferior outcomes compared with those who underwent direct surgery in terms of 5-year disease-free survival (Log rank test: P = 0.083, Breslow test: P = 0.089). The two groups also exhibited no significant differences statistically in the context of overall survival (Log rank test: P = 0.652, Breslow test: P = 0.758).
Conclusion: Completion surgery is a safe and feasible treatment option for T1 colorectal adenocarcinoma patients with high-risk factors, particularly those with deep submucosal invasion and vascular or lymphatic invasion following endoscopic treatment. Furthermore, subsequent treatment should be chosen based on a comprehensive analysis of the patient's history of abdominal surgery, willingness, and pathological features.
期刊介绍:
The Journal of Gastrointestinal Cancer is a multidisciplinary medium for the publication of novel research pertaining to cancers arising from the gastrointestinal tract.The journal is dedicated to the most rapid publication possible.The journal publishes papers in all relevant fields, emphasizing those studies that are helpful in understanding and treating cancers affecting the esophagus, stomach, liver, gallbladder and biliary tree, pancreas, small bowel, large bowel, rectum, and anus. In addition, the Journal of Gastrointestinal Cancer publishes basic and translational scientific information from studies providing insight into the etiology and progression of cancers affecting these organs. New insights are provided from diverse areas of research such as studies exploring pre-neoplastic states, risk factors, epidemiology, genetics, preclinical therapeutics, surgery, radiation therapy, novel medical therapeutics, clinical trials, and outcome studies.In addition to reports of original clinical and experimental studies, the journal also publishes: case reports, state-of-the-art reviews on topics of immediate interest or importance; invited articles analyzing particular areas of pancreatic research and knowledge; perspectives in which critical evaluation and conflicting opinions about current topics may be expressed; meeting highlights that summarize important points presented at recent meetings; abstracts of symposia and conferences; book reviews; hypotheses; Letters to the Editors; and other items of special interest, including:Complex Cases in GI Oncology: This is a new initiative to provide a forum to review and discuss the history and management of complex and involved gastrointestinal oncology cases. The format will be similar to a teaching case conference where a case vignette is presented and is followed by a series of questions and discussion points. A brief reference list supporting the points made in discussion would be expected.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
