Patients undergoing a prior failed attempt of chronic total occlusion-percutaneous coronary intervention (CTO-PCI) represent a challenging subgroup across all patients undergoing CTO-PCI. There are limited data on the effects of a prior failed attempt on the outcomes of subsequent CTO-PCI. We aimed to compare the procedural results and 24-month outcomes of prior-failed-attempt CTO-PCI with those of initial-attempt CTO-PCI.
Patients who underwent attempted CTO-PCI between January 2017 and December 2019 were prospectively enrolled. We analyzed the procedural results and 24-month major adverse cardiac events (MACE) between patients who underwent prior-failed-attempt and initial-attempt CTO-PCI. MACE was defined as a composite of cardiac death, target vessel-related myocardial infarction, and ischemia-driven target vessel revascularization (TVR) during follow-up.
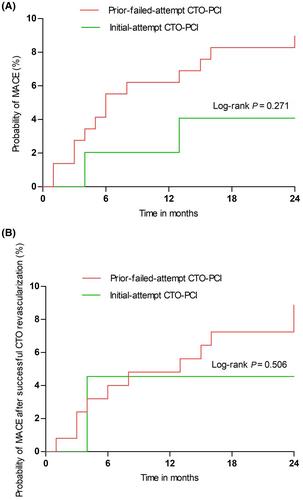
In total, 484 patients who underwent CTO-PCI (prior-failed-attempt, n = 49; initial-attempt, n = 435) were enrolled during the study period. After propensity score matching (1:3), 147 patients were included in the initial-attempt group. The proportion of the Japanese-CTO (J-CTO) score ≥2 was higher in the patients who underwent prior failed attempt than in those who underwent initial attempt (77.5% vs. 38.8%, p < 0.001). The retrograde approach was more often adopted in the prior-failed-attempt group than in the initial-attempt group (32.7% vs. 3.4%, [P< 0.001). Successful CTO revascularization rates were significantly lower in the prior-failed attempt-group than in the initial attempt group (53.1% vs. 83.3%, P < 0.001). The multivariate analysis revealed that J-CTO score ≥2 [odds ratio (OR), 0.359; 95% confidence interval (CI), 0.159–0.812; P = 0.014], intravascular ultrasound procedure (OR, 4.640; 95% CI, 1.380–15.603; P = 0.013), and prior failed attempt (OR, 0.285; 95% CI, 0.125–0.648; P = 0.003) were the independent predictors for successful CTO revascularization. There were no significant differences in major procedural complications (2.0% vs. 0.7%, p = 0.438) and MACE rates (4.1% vs. 8.8%, p = 0.438) between the groups, mainly due to the TVR rate (4.1% vs. 8.2%, P = 0.522).
Compared with initial-attempt CTO-PCI, prior-failed-attempt CTO-PCI deserves more attention, since it is associated with a lower successful CTO revascularization rate. Prior failed attempt, J-CTO score ≥2, and IVUS procedure are the determining factors for predicting successful CTO revascularization. There are no significantly different unfavorable outcomes between patients who undergo prior-failed-attempt and initial-attempt CTO-PCI.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
