{"title":"Does Wastewater Analysis Play a Role in Tracking Colorectal Cancer Hot Spots to Guide Geotargeted Neighborhood Interventions?","authors":"Allie Jin, Rochelle H. Holm, Ted Smith, Natalie DuPré, Sandra Kavalukas","doi":"10.1021/acsestwater.4c00641","DOIUrl":null,"url":null,"abstract":"Wastewater has been used as an early warning system to detect infectious disease outbreaks. (1,2) Extending this platform to monitor and survey areas with increased environmental health risks, such as volatile organic compound metabolites, (3) remains an unexplored opportunity. Globally, colorectal cancer (CRC) is ranked third for most common incidence and second for cancer-related mortality. (4,5) Despite a decline in CRC incidence rates among individuals who are ≥65 years of age (attributed largely to screening efforts), cases of early onset CRC (patients who are <50 years of age) are rapidly increasing, with the projected incidence rate doubling by 2030. (6) Talibov et al. (7) showed that exposure to volatile organic compounds in occupational settings was positively associated with CRC. Many high-risk populations that may be exposed to these compounds remain unscreened due healthcare disparities or due to age-related guidelines, (8) yet wastewater catches all ages. We advocate for further research aimed at integrating population-level environmental toxin wastewater data with existing patient and environmental health data sets to identify and track CRC hot spots and guide community-based interventions to decrease the incidence of CRC (Figure 1). Figure 1. Framework to enable better tracking of colorectal cancer hot spots with paired wastewater surveillance, ambient air monitoring, known registries, and biospecimens. Wastewater-based epidemiology provides an established approach for surveilling various population-sized areas, and its role in cancer hot spot tracking might be best at the neighborhood scale. A disproportionate number of patients with CRC residing in specific geographic areas may present to their local medical centers. Epidemiologists can monitor the CRC incidence rates using state cancer databases and integrate these rates with reports on ambient levels of environmental toxins. Biospecimens from patients with CRC residing within these identified areas can be triangulated with anonymous community-level wastewater samples for environmental pollutants that are geographically bound to neighborhood hot spots. Despite the overall increase in CRC screening rates, disparities persist in low-income communities and racially marginalized populations. (8) These populations experience higher levels of exposure to known environmental pollutants and barriers to access preventive and interventional healthcare services. A wastewater-based approach may allow for an increased intensity of community-level surveilling of populations at risk of CRC, including directed patient evaluations and CRC screening. This is analogous to SARS-CoV-2 infection testing, in which SARS-CoV-2 personal testing was inequitable and wastewater evaluation for SARS-CoV-2 enabled more equitable screening at a population level that informed neighborhood trends, even before COVID-19 symptoms became noticeable. Environmental surveillance data from wastewater may also provide insights into the lifetime environmental burdens that increase the risk of CRC. Wastewater evaluation of environmental carcinogens provides an additional avenue for cancer prevention. Residential proximity to industrial pollution sources has been attributed to CRC risk, presenting danger for the entire surrounding population instead of the historically described industrial workers. (9) Wastewater sampling allows the collection of data from defined geographic zones within communities, regardless of whether residents have pursued cancer screening or treatment or whether the onset is early or late, to promote CRC screening in such areas. By surveilling environmental carcinogens, as opposed to burdening the individual to overcome the structural barriers to CRC screening, public health departments can monitor and limit sources of environmental carcinogens, particularly in the neighborhoods that are known CRC hot spots. Wastewater may be a novel solution to CRC disparities with associated environmental injustices. Utilizing wastewater as an additional data source for CRC monitoring may not warrant the precision of lead time that was urgently needed during the COVID-19 pandemic. (1) It is unlikely that such an amount of data is needed for CRC monitoring; a yearly environmental toxin sample to guide geographic boundaries for community-based intervention may be most appropriate. Anderson et al. (10) reported neighborhood-level increased SARS-CoV-2 wastewater concentrations, leading to the successful implementation of a geotargeted advertising intervention to boost COVID-19 vaccination rates in high-risk neighborhoods. A complementary approach for CRC could be adopted to screen environmental toxins in wastewater and, when paired with ambient air monitoring, known registries, and biospecimens, alert geotargeted residents to their increased risk of developing CRC. With the added value of quantitative wastewater data, physicians can further enhance awareness by developing localized and culturally appropriate prevention strategies or by bolstering screening efforts. Collaborating with local organizations, cancer advocacy organizations can prioritize limited resources for planning and executing relevant and impactful yearly interventions in community zones rather than a uniform citywide intervention. Grassroots organizations can further advocate for their residents’ day-to-day health by backing initiatives for stricter control of industrial emissions and environmental cleanup efforts. Budget meetings also provide a platform for highlighting the importance of access to green spaces, nutritious foods, and affordable CRC screening, which work together to decrease the CRC burden on communities. Wastewater surveillance has the potential to be used in other public health areas, including cancer, particularly in urban areas with piped sewer networks. Wastewater may play a novel role in overcoming CRC racial and income disparities and the use of hot spot data to promote screening in neighborhoods that have less access to healthcare and include historically marginalized populations. CRC presents a significant public health challenge in the United States, particularly in early onset patients who are <50 years of age. The additive value of wastewater analysis provides a strong benefit for transdisciplinary integration by epidemiologists, physicians, environmental scientists, public health practitioners, and geographic researchers to stop, or at least slow, the increase in the number of CRC hot spots. T.S., N.D., and S.K. are joint senior authors. A.J. and R.H.H. drafted the article. All authors were involved in manuscript editing and were responsible for the decision to submit for publication. The University of Louisville Institutional Review Board approved this research as Human Subjects Research (IRB 23.0319). There is no patient/participant information included in this work, and thus, no applicable written informed consent was warranted. Rochelle H. Holm is an associate professor with the Christina Lee Brown Envirome Institute at the University of Louisville. Her current research includes surveillance of pathogen and environmental toxins across sewered and nonsewered sanitation systems. This work was supported by the Owsley Brown II Family Foundation, the NIH NIEHS University of Louisville (UofL) Center for Integrative Environmental Health Sciences (CIEHS) (P30 ES030283, N.D.), and UofL NIEHS Superfund Grant P42 ES023716 (N.D.). This article references 10 other publications. This article has not yet been cited by other publications.","PeriodicalId":7078,"journal":{"name":"ACS Es&t Water","volume":"44 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-08-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Es&t Water","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1021/acsestwater.4c00641","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
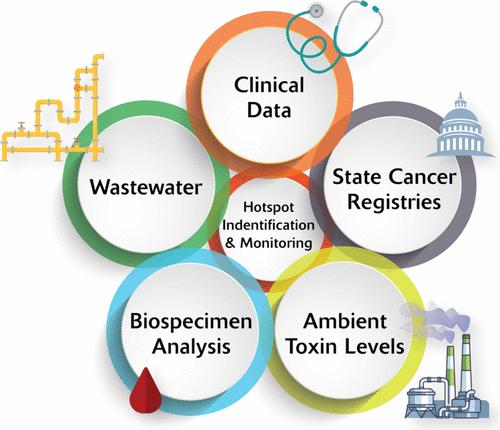
Wastewater has been used as an early warning system to detect infectious disease outbreaks. (1,2) Extending this platform to monitor and survey areas with increased environmental health risks, such as volatile organic compound metabolites, (3) remains an unexplored opportunity. Globally, colorectal cancer (CRC) is ranked third for most common incidence and second for cancer-related mortality. (4,5) Despite a decline in CRC incidence rates among individuals who are ≥65 years of age (attributed largely to screening efforts), cases of early onset CRC (patients who are <50 years of age) are rapidly increasing, with the projected incidence rate doubling by 2030. (6) Talibov et al. (7) showed that exposure to volatile organic compounds in occupational settings was positively associated with CRC. Many high-risk populations that may be exposed to these compounds remain unscreened due healthcare disparities or due to age-related guidelines, (8) yet wastewater catches all ages. We advocate for further research aimed at integrating population-level environmental toxin wastewater data with existing patient and environmental health data sets to identify and track CRC hot spots and guide community-based interventions to decrease the incidence of CRC (Figure 1). Figure 1. Framework to enable better tracking of colorectal cancer hot spots with paired wastewater surveillance, ambient air monitoring, known registries, and biospecimens. Wastewater-based epidemiology provides an established approach for surveilling various population-sized areas, and its role in cancer hot spot tracking might be best at the neighborhood scale. A disproportionate number of patients with CRC residing in specific geographic areas may present to their local medical centers. Epidemiologists can monitor the CRC incidence rates using state cancer databases and integrate these rates with reports on ambient levels of environmental toxins. Biospecimens from patients with CRC residing within these identified areas can be triangulated with anonymous community-level wastewater samples for environmental pollutants that are geographically bound to neighborhood hot spots. Despite the overall increase in CRC screening rates, disparities persist in low-income communities and racially marginalized populations. (8) These populations experience higher levels of exposure to known environmental pollutants and barriers to access preventive and interventional healthcare services. A wastewater-based approach may allow for an increased intensity of community-level surveilling of populations at risk of CRC, including directed patient evaluations and CRC screening. This is analogous to SARS-CoV-2 infection testing, in which SARS-CoV-2 personal testing was inequitable and wastewater evaluation for SARS-CoV-2 enabled more equitable screening at a population level that informed neighborhood trends, even before COVID-19 symptoms became noticeable. Environmental surveillance data from wastewater may also provide insights into the lifetime environmental burdens that increase the risk of CRC. Wastewater evaluation of environmental carcinogens provides an additional avenue for cancer prevention. Residential proximity to industrial pollution sources has been attributed to CRC risk, presenting danger for the entire surrounding population instead of the historically described industrial workers. (9) Wastewater sampling allows the collection of data from defined geographic zones within communities, regardless of whether residents have pursued cancer screening or treatment or whether the onset is early or late, to promote CRC screening in such areas. By surveilling environmental carcinogens, as opposed to burdening the individual to overcome the structural barriers to CRC screening, public health departments can monitor and limit sources of environmental carcinogens, particularly in the neighborhoods that are known CRC hot spots. Wastewater may be a novel solution to CRC disparities with associated environmental injustices. Utilizing wastewater as an additional data source for CRC monitoring may not warrant the precision of lead time that was urgently needed during the COVID-19 pandemic. (1) It is unlikely that such an amount of data is needed for CRC monitoring; a yearly environmental toxin sample to guide geographic boundaries for community-based intervention may be most appropriate. Anderson et al. (10) reported neighborhood-level increased SARS-CoV-2 wastewater concentrations, leading to the successful implementation of a geotargeted advertising intervention to boost COVID-19 vaccination rates in high-risk neighborhoods. A complementary approach for CRC could be adopted to screen environmental toxins in wastewater and, when paired with ambient air monitoring, known registries, and biospecimens, alert geotargeted residents to their increased risk of developing CRC. With the added value of quantitative wastewater data, physicians can further enhance awareness by developing localized and culturally appropriate prevention strategies or by bolstering screening efforts. Collaborating with local organizations, cancer advocacy organizations can prioritize limited resources for planning and executing relevant and impactful yearly interventions in community zones rather than a uniform citywide intervention. Grassroots organizations can further advocate for their residents’ day-to-day health by backing initiatives for stricter control of industrial emissions and environmental cleanup efforts. Budget meetings also provide a platform for highlighting the importance of access to green spaces, nutritious foods, and affordable CRC screening, which work together to decrease the CRC burden on communities. Wastewater surveillance has the potential to be used in other public health areas, including cancer, particularly in urban areas with piped sewer networks. Wastewater may play a novel role in overcoming CRC racial and income disparities and the use of hot spot data to promote screening in neighborhoods that have less access to healthcare and include historically marginalized populations. CRC presents a significant public health challenge in the United States, particularly in early onset patients who are <50 years of age. The additive value of wastewater analysis provides a strong benefit for transdisciplinary integration by epidemiologists, physicians, environmental scientists, public health practitioners, and geographic researchers to stop, or at least slow, the increase in the number of CRC hot spots. T.S., N.D., and S.K. are joint senior authors. A.J. and R.H.H. drafted the article. All authors were involved in manuscript editing and were responsible for the decision to submit for publication. The University of Louisville Institutional Review Board approved this research as Human Subjects Research (IRB 23.0319). There is no patient/participant information included in this work, and thus, no applicable written informed consent was warranted. Rochelle H. Holm is an associate professor with the Christina Lee Brown Envirome Institute at the University of Louisville. Her current research includes surveillance of pathogen and environmental toxins across sewered and nonsewered sanitation systems. This work was supported by the Owsley Brown II Family Foundation, the NIH NIEHS University of Louisville (UofL) Center for Integrative Environmental Health Sciences (CIEHS) (P30 ES030283, N.D.), and UofL NIEHS Superfund Grant P42 ES023716 (N.D.). This article references 10 other publications. This article has not yet been cited by other publications.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
