Rebecca A. Shatsky, Meghna S. Trivedi, Christina Yau, Rita Nanda, Hope S. Rugo, Marie Davidian, Butch Tsiatis, Anne M. Wallace, A. Jo Chien, Erica Stringer-Reasor, Judy C. Boughey, Coral Omene, Mariya Rozenblit, Kevin Kalinsky, Anthony D. Elias, Christos Vaklavas, Heather Beckwith, Nicole Williams, Mili Arora, Chaitali Nangia, Evanthia T. Roussos Torres, Brittani Thomas, Kathy S. Albain, Amy S. Clark, Carla Falkson, Dawn L. Hershman, Claudine Isaacs, Alexandra Thomas, Jennifer Tseng, Amy Sanford, Kay Yeung, Sarah Boles, Yunni Yi Chen, Laura Huppert, Nusrat Jahan, Catherine Parker, Karthik Giridhar, Frederick M. Howard, M. Michele Blackwood, Tara Sanft, Wen Li, Natsuko Onishi, Adam L. Asare, Philip Beineke, Peter Norwood, Lamorna Brown-Swigart, Gillian L. Hirst, Jeffrey B. Matthews, Brian Moore, W. Fraser Symmans, Elissa Price, Diane Heditsian, Barbara LeStage, Jane Perlmutter, Paula Pohlmann, Angela DeMichele, Douglas Yee, Laura J. van ’t Veer, Nola M. Hylton, Laura J. Esserman
{"title":"Datopotamab–deruxtecan plus durvalumab in early-stage breast cancer: the sequential multiple assignment randomized I-SPY2.2 phase 2 trial","authors":"Rebecca A. Shatsky, Meghna S. Trivedi, Christina Yau, Rita Nanda, Hope S. Rugo, Marie Davidian, Butch Tsiatis, Anne M. Wallace, A. Jo Chien, Erica Stringer-Reasor, Judy C. Boughey, Coral Omene, Mariya Rozenblit, Kevin Kalinsky, Anthony D. Elias, Christos Vaklavas, Heather Beckwith, Nicole Williams, Mili Arora, Chaitali Nangia, Evanthia T. Roussos Torres, Brittani Thomas, Kathy S. Albain, Amy S. Clark, Carla Falkson, Dawn L. Hershman, Claudine Isaacs, Alexandra Thomas, Jennifer Tseng, Amy Sanford, Kay Yeung, Sarah Boles, Yunni Yi Chen, Laura Huppert, Nusrat Jahan, Catherine Parker, Karthik Giridhar, Frederick M. Howard, M. Michele Blackwood, Tara Sanft, Wen Li, Natsuko Onishi, Adam L. Asare, Philip Beineke, Peter Norwood, Lamorna Brown-Swigart, Gillian L. Hirst, Jeffrey B. Matthews, Brian Moore, W. Fraser Symmans, Elissa Price, Diane Heditsian, Barbara LeStage, Jane Perlmutter, Paula Pohlmann, Angela DeMichele, Douglas Yee, Laura J. van ’t Veer, Nola M. Hylton, Laura J. Esserman","doi":"10.1038/s41591-024-03267-1","DOIUrl":null,"url":null,"abstract":"Sequential adaptive trial designs can help accomplish the goals of personalized medicine, optimizing outcomes and avoiding unnecessary toxicity. Here we describe the results of incorporating a promising antibody–drug conjugate, datopotamab–deruxtecan (Dato-DXd) in combination with programmed cell death-ligand 1 inhibitor, durvalumab, as the first sequence of therapy in the I-SPY2.2 phase 2 neoadjuvant sequential multiple assignment randomization trial for high-risk stage 2/3 breast cancer. The trial includes three blocks of treatment, with initial randomization to different experimental agent(s) (block A), followed by a taxane-based regimen tailored to tumor subtype (block B), followed by doxorubicin–cyclophosphamide (block C). Subtype-specific algorithms based on magnetic resonance imaging volume change and core biopsy guide treatment redirection after each block, including the option of early surgical resection in patients predicted to have a high likelihood of pathologic complete response, which is the primary endpoint assessed when resection occurs. There are two primary efficacy analyses: after block A and across all blocks for six prespecified HER2-negative subtypes (defined by hormone receptor status and/or response-predictive subtypes). In total, 106 patients were treated with Dato-DXd/durvalumab in block A. In the immune-positive subtype, Dato-DXd/durvalumab exceeded the prespecified threshold for success (graduated) after block A; and across all blocks, pathologic complete response rates were equivalent to the rate expected for the standard of care (79%), but 54% achieved that result after Dato-DXd/durvalumab alone (block A) and 92% without doxorubicin–cyclophosphamide (after blocks A + B). The treatment strategy across all blocks graduated in the hormone-negative/immune-negative subtype. No new toxicities were observed. Stomatitis was the most common side effect in block A. No patients receiving block A treatment alone had adrenal insufficiency. Dato-DXd/durvalumab is a promising therapy combination that can eliminate standard chemotherapy in many patients, particularly the immune-positive subtype. ClinicalTrials.gov registration: NCT01042379 . In the I-SPY2.2 trial, patients with high-risk stage 2/3 breast cancer received neoadjuvant datopotamab–deruxtecan plus durvalumab, followed by sequential chemotherapy with or without targeted therapy, with the option of early surgical resection after each block of therapy, showing that de-escalation of therapy is possible for several patient subgroups without compromising outcome and avoiding toxicity of standard chemotherapy.","PeriodicalId":19037,"journal":{"name":"Nature Medicine","volume":"30 12","pages":"3737-3747"},"PeriodicalIF":50.0000,"publicationDate":"2024-09-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nature Medicine","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s41591-024-03267-1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
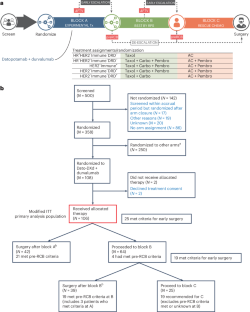
Sequential adaptive trial designs can help accomplish the goals of personalized medicine, optimizing outcomes and avoiding unnecessary toxicity. Here we describe the results of incorporating a promising antibody–drug conjugate, datopotamab–deruxtecan (Dato-DXd) in combination with programmed cell death-ligand 1 inhibitor, durvalumab, as the first sequence of therapy in the I-SPY2.2 phase 2 neoadjuvant sequential multiple assignment randomization trial for high-risk stage 2/3 breast cancer. The trial includes three blocks of treatment, with initial randomization to different experimental agent(s) (block A), followed by a taxane-based regimen tailored to tumor subtype (block B), followed by doxorubicin–cyclophosphamide (block C). Subtype-specific algorithms based on magnetic resonance imaging volume change and core biopsy guide treatment redirection after each block, including the option of early surgical resection in patients predicted to have a high likelihood of pathologic complete response, which is the primary endpoint assessed when resection occurs. There are two primary efficacy analyses: after block A and across all blocks for six prespecified HER2-negative subtypes (defined by hormone receptor status and/or response-predictive subtypes). In total, 106 patients were treated with Dato-DXd/durvalumab in block A. In the immune-positive subtype, Dato-DXd/durvalumab exceeded the prespecified threshold for success (graduated) after block A; and across all blocks, pathologic complete response rates were equivalent to the rate expected for the standard of care (79%), but 54% achieved that result after Dato-DXd/durvalumab alone (block A) and 92% without doxorubicin–cyclophosphamide (after blocks A + B). The treatment strategy across all blocks graduated in the hormone-negative/immune-negative subtype. No new toxicities were observed. Stomatitis was the most common side effect in block A. No patients receiving block A treatment alone had adrenal insufficiency. Dato-DXd/durvalumab is a promising therapy combination that can eliminate standard chemotherapy in many patients, particularly the immune-positive subtype. ClinicalTrials.gov registration: NCT01042379 . In the I-SPY2.2 trial, patients with high-risk stage 2/3 breast cancer received neoadjuvant datopotamab–deruxtecan plus durvalumab, followed by sequential chemotherapy with or without targeted therapy, with the option of early surgical resection after each block of therapy, showing that de-escalation of therapy is possible for several patient subgroups without compromising outcome and avoiding toxicity of standard chemotherapy.
期刊介绍:
Nature Medicine is a monthly journal publishing original peer-reviewed research in all areas of medicine. The publication focuses on originality, timeliness, interdisciplinary interest, and the impact on improving human health. In addition to research articles, Nature Medicine also publishes commissioned content such as News, Reviews, and Perspectives. This content aims to provide context for the latest advances in translational and clinical research, reaching a wide audience of M.D. and Ph.D. readers. All editorial decisions for the journal are made by a team of full-time professional editors.
Nature Medicine consider all types of clinical research, including:
-Case-reports and small case series
-Clinical trials, whether phase 1, 2, 3 or 4
-Observational studies
-Meta-analyses
-Biomarker studies
-Public and global health studies
Nature Medicine is also committed to facilitating communication between translational and clinical researchers. As such, we consider “hybrid” studies with preclinical and translational findings reported alongside data from clinical studies.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
