Comparative incidence and risk factors for gastrointestinal bleeding following percutaneous coronary intervention for coronary artery disease: Insights from the Keio Cardiovascular Registry in Japan
{"title":"Comparative incidence and risk factors for gastrointestinal bleeding following percutaneous coronary intervention for coronary artery disease: Insights from the Keio Cardiovascular Registry in Japan","authors":"Ikuko Ueda , Shun Kohsaka , Yohei Numasawa , Ryo Takemura , Naoki Hosoe , Masaki Ieda","doi":"10.1016/j.thromres.2024.109150","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>In patients with coronary artery disease (CAD) undergoing percutaneous coronary intervention (PCI), antiplatelet medication usage is crucial for preventing thrombotic events. However, it requires careful monitoring, especially because of the risk of life-threatening bleeding complications. In hemorrhagic complications, assessment of patient background and risk of gastrointestinal bleeding (GIB) remain limited for GIB that develops during long-term observation after hospital discharge. This study aimed to examine the incidence of GIB and patient characteristics in CAD post-PCI.</p></div><div><h3>Methods</h3><p>All CAD patients undergoing PCI for urgent, emergent, or elective indications were enrolled in the Keio Interhospital Cardiovascular Studies (JCD-KiCS)-PCI registry (January 2009 and December 2017) and followed up to 2 years after PCI discharge. From the JCD-KiCS PCI registry, 8864 patients (median [interquartile range [IQR]] age: non-GIB: 69.0 y [16 y], upper GIB (UGI): 72.0 y [15.5 y], lower GIB (LGI): 73.0 y [IQR: 13 y]) were categorized based on the occurrence of hospitalization-requiring GIB. Patient characteristics and detailed information regarding these GIB events, including the location (upper vs lower GI) and bleeding severity, were analyzed.</p></div><div><h3>Results</h3><p>Overall, 36 patients experienced UGI, while 85 patients experienced LGI. The rates of dual antiplatelet therapy (DAPT) and triple therapy were significantly different among the non-GIB (n = 8734), UGI (n = 36) and LGI (n = 85) groups (DAPT [aspirin + P2Y12 (clopidogrel/prasugrel/ticlopidine)]: 64 [76.2 %] in the LGI group vs 24 [68.6 %] in the UGI group vs 7330 [84.6 %] in the non-GIB group; triple therapy [aspirin + P2Y12 (clopidogrel/prasugrel/ticlopidine)] + oral anticoagulant (OAC) (warfarin/direct oral anticoagulant [DOAC]): 17 [20.2 %] in the LGI group vs 8 [22.9 %] in the UGI group vs 836 [9.6 %] in the non-GIB group; p < 0.001). In the LGI and UGI groups, aspirin and warfarin were used in 2 (2.4 %) and 2 (5.7 %) patients, respectively, but not in combination with DOAC. The 2-year post-PCI hospitalization incidence for GIB was 1.4 % (LGI, 1.0 %; UGI, 0.4 %). The most common causes were colonic diverticular hemorrhage (43.5 %) for LGI and duodenal ulcer (21.9 %) for UGI. No significant differences were found in the cumulative 2-year post-PCI risks between the LGI and UGI groups (log-rank p = 0.97). Most GIB events were Bleeding Academic Research Consortium 2-equivalent (hemoglobin decrease <3 g/dL). Notably, the use of OACs at PCI discharge, bleeding complications within 72 h, and preprocedural anemia were significantly correlated with an increased GIB risk.</p></div><div><h3>Conclusions</h3><p>The real-world incidence of LGI is two times higher than that of UGI in CAD patients undergoing PCI, and most events are mild. OAC use at PCI discharge is the strongest potential risk factor for GIB development.</p></div>","PeriodicalId":23064,"journal":{"name":"Thrombosis research","volume":"243 ","pages":"Article 109150"},"PeriodicalIF":3.4000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S0049384824002822/pdfft?md5=183c1e641cf929263bc192156fd36c12&pid=1-s2.0-S0049384824002822-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thrombosis research","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0049384824002822","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/12 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
In patients with coronary artery disease (CAD) undergoing percutaneous coronary intervention (PCI), antiplatelet medication usage is crucial for preventing thrombotic events. However, it requires careful monitoring, especially because of the risk of life-threatening bleeding complications. In hemorrhagic complications, assessment of patient background and risk of gastrointestinal bleeding (GIB) remain limited for GIB that develops during long-term observation after hospital discharge. This study aimed to examine the incidence of GIB and patient characteristics in CAD post-PCI.
Methods
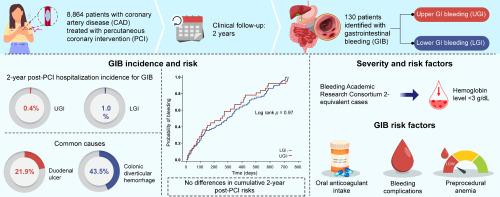
All CAD patients undergoing PCI for urgent, emergent, or elective indications were enrolled in the Keio Interhospital Cardiovascular Studies (JCD-KiCS)-PCI registry (January 2009 and December 2017) and followed up to 2 years after PCI discharge. From the JCD-KiCS PCI registry, 8864 patients (median [interquartile range [IQR]] age: non-GIB: 69.0 y [16 y], upper GIB (UGI): 72.0 y [15.5 y], lower GIB (LGI): 73.0 y [IQR: 13 y]) were categorized based on the occurrence of hospitalization-requiring GIB. Patient characteristics and detailed information regarding these GIB events, including the location (upper vs lower GI) and bleeding severity, were analyzed.
Results
Overall, 36 patients experienced UGI, while 85 patients experienced LGI. The rates of dual antiplatelet therapy (DAPT) and triple therapy were significantly different among the non-GIB (n = 8734), UGI (n = 36) and LGI (n = 85) groups (DAPT [aspirin + P2Y12 (clopidogrel/prasugrel/ticlopidine)]: 64 [76.2 %] in the LGI group vs 24 [68.6 %] in the UGI group vs 7330 [84.6 %] in the non-GIB group; triple therapy [aspirin + P2Y12 (clopidogrel/prasugrel/ticlopidine)] + oral anticoagulant (OAC) (warfarin/direct oral anticoagulant [DOAC]): 17 [20.2 %] in the LGI group vs 8 [22.9 %] in the UGI group vs 836 [9.6 %] in the non-GIB group; p < 0.001). In the LGI and UGI groups, aspirin and warfarin were used in 2 (2.4 %) and 2 (5.7 %) patients, respectively, but not in combination with DOAC. The 2-year post-PCI hospitalization incidence for GIB was 1.4 % (LGI, 1.0 %; UGI, 0.4 %). The most common causes were colonic diverticular hemorrhage (43.5 %) for LGI and duodenal ulcer (21.9 %) for UGI. No significant differences were found in the cumulative 2-year post-PCI risks between the LGI and UGI groups (log-rank p = 0.97). Most GIB events were Bleeding Academic Research Consortium 2-equivalent (hemoglobin decrease <3 g/dL). Notably, the use of OACs at PCI discharge, bleeding complications within 72 h, and preprocedural anemia were significantly correlated with an increased GIB risk.
Conclusions
The real-world incidence of LGI is two times higher than that of UGI in CAD patients undergoing PCI, and most events are mild. OAC use at PCI discharge is the strongest potential risk factor for GIB development.
期刊介绍:
Thrombosis Research is an international journal dedicated to the swift dissemination of new information on thrombosis, hemostasis, and vascular biology, aimed at advancing both science and clinical care. The journal publishes peer-reviewed original research, reviews, editorials, opinions, and critiques, covering both basic and clinical studies. Priority is given to research that promises novel approaches in the diagnosis, therapy, prognosis, and prevention of thrombotic and hemorrhagic diseases.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
