Therapeutic strategies and treatment sequencing in patients with chronic lymphocytic leukemia: An international study of ERIC, the European Research Initiative on CLL
Thomas Chatzikonstantinou, Lydia Scarfò, Eva Minga, Georgios Karakatsoulis, Dimitra Chamou, Jana Kotaskova, Gloria Iacoboni, Christos Demosthenous, Elisa Albi, Miguel Alcoceba, Salem Al-Shemari, Thérèse Aurran-Schleinitz, Francesca Bacchiarri, Sofia Chatzileontiadou, Rosa Collado, Zadie Davis, Marcos Daniel de Deus Santos, Maria Dimou, Elena Dmitrieva, David Donaldson, Gimena Dos Santos, Barbara Dreta, Maria Efstathopoulou, Shaimaa El-Ashwah, Alicia Enrico, Andrzej Frygier, Sara Galimberti, Andrea Galitzia, Eva Gimeno, Valerio Guarente, Romain Guieze, Sean Harrop, Eleftheria Hatzimichael, Yair Herishanu, José-Ángel Hernández-Rivas, Ozren Jaksic, Elżbieta Kalicińska, Kamel Laribi, Volkan Karakus, Arnon P. Kater, Bonnie Kho, Maria Kislova, Εliana Konstantinou, Maya Koren-Michowitz, Ioannis Kotsianidis, Zuzana Kubova, Jorge Labrador, Deepesh Lad, Luca Laurenti, Thomas Longval, Alberto Lopez-Garcia, Juan Marquet, Stanislava Maslejova, Carlota Mayor-Bastida, Biljana Mihaljevic, Ivana Milosevic, Fatima Miras, Riccardo Moia, Marta Morawska, Uttam K. Nath, Almudena Navarro-Bailón, Jacopo Olivieri, Irina Panovska-Stavridis, Maria Papaioannou, Cheyenne Pierie, Anna Puiggros, Gianluigi Reda, Gian M. Rigolin, Rosa Ruchlemer, Mattia Schipani, Annett Schiwitza, Yandong Shen, Tereza Shokralla, Martin Simkovic, Svetlana Smirnova, Dina S. A. Soliman, Stephan Stilgenbauer, Tamar Tadmor, Kristina Tomic, Eric Tse, Theodoros Vassilakopoulos, Andrea Visentin, Candida Vitale, George Vrachiolias, Vojin Vukovic, Renata Walewska, Zhenshu Xu, Munci Yagci, Lucrecia Yañez, Mohamed Yassin, Jana Zuchnicka, David Oscier, Alessandro Gozzetti, Panagiotis Panagiotidis, Francesc Bosch, Paolo Sportoletti, Blanca Espinet, Gerassimos A. Pangalis, Viola M. Popov, Stephen Mulligan, Maria Angelopoulou, Fatih Demirkan, Tomas Papajík, Bella Biderman, Roberta Murru, Marta Coscia, Constantine Tam, Antonio Cuneo, Gianluca Gaidano, Rainer Claus, Niki Stavroyianni, Livio Trentin, Darko Antic, Lukas Smolej, Olga B. Kalashnikova, Mark Catherwood, Martin Spacek, Sarka Pospisilova, Michael Doubek, Eugene Nikitin, Anastasia Chatzidimitriou, Paolo Ghia, Kostas Stamatopoulos
{"title":"Therapeutic strategies and treatment sequencing in patients with chronic lymphocytic leukemia: An international study of ERIC, the European Research Initiative on CLL","authors":"Thomas Chatzikonstantinou, Lydia Scarfò, Eva Minga, Georgios Karakatsoulis, Dimitra Chamou, Jana Kotaskova, Gloria Iacoboni, Christos Demosthenous, Elisa Albi, Miguel Alcoceba, Salem Al-Shemari, Thérèse Aurran-Schleinitz, Francesca Bacchiarri, Sofia Chatzileontiadou, Rosa Collado, Zadie Davis, Marcos Daniel de Deus Santos, Maria Dimou, Elena Dmitrieva, David Donaldson, Gimena Dos Santos, Barbara Dreta, Maria Efstathopoulou, Shaimaa El-Ashwah, Alicia Enrico, Andrzej Frygier, Sara Galimberti, Andrea Galitzia, Eva Gimeno, Valerio Guarente, Romain Guieze, Sean Harrop, Eleftheria Hatzimichael, Yair Herishanu, José-Ángel Hernández-Rivas, Ozren Jaksic, Elżbieta Kalicińska, Kamel Laribi, Volkan Karakus, Arnon P. Kater, Bonnie Kho, Maria Kislova, Εliana Konstantinou, Maya Koren-Michowitz, Ioannis Kotsianidis, Zuzana Kubova, Jorge Labrador, Deepesh Lad, Luca Laurenti, Thomas Longval, Alberto Lopez-Garcia, Juan Marquet, Stanislava Maslejova, Carlota Mayor-Bastida, Biljana Mihaljevic, Ivana Milosevic, Fatima Miras, Riccardo Moia, Marta Morawska, Uttam K. Nath, Almudena Navarro-Bailón, Jacopo Olivieri, Irina Panovska-Stavridis, Maria Papaioannou, Cheyenne Pierie, Anna Puiggros, Gianluigi Reda, Gian M. Rigolin, Rosa Ruchlemer, Mattia Schipani, Annett Schiwitza, Yandong Shen, Tereza Shokralla, Martin Simkovic, Svetlana Smirnova, Dina S. A. Soliman, Stephan Stilgenbauer, Tamar Tadmor, Kristina Tomic, Eric Tse, Theodoros Vassilakopoulos, Andrea Visentin, Candida Vitale, George Vrachiolias, Vojin Vukovic, Renata Walewska, Zhenshu Xu, Munci Yagci, Lucrecia Yañez, Mohamed Yassin, Jana Zuchnicka, David Oscier, Alessandro Gozzetti, Panagiotis Panagiotidis, Francesc Bosch, Paolo Sportoletti, Blanca Espinet, Gerassimos A. Pangalis, Viola M. Popov, Stephen Mulligan, Maria Angelopoulou, Fatih Demirkan, Tomas Papajík, Bella Biderman, Roberta Murru, Marta Coscia, Constantine Tam, Antonio Cuneo, Gianluca Gaidano, Rainer Claus, Niki Stavroyianni, Livio Trentin, Darko Antic, Lukas Smolej, Olga B. Kalashnikova, Mark Catherwood, Martin Spacek, Sarka Pospisilova, Michael Doubek, Eugene Nikitin, Anastasia Chatzidimitriou, Paolo Ghia, Kostas Stamatopoulos","doi":"10.1002/hem3.70004","DOIUrl":null,"url":null,"abstract":"<p>Novel small molecule inhibitors have revolutionized the treatment of chronic lymphocytic leukemia (CLL). Indeed, BTK (BTKi) and BCL2 inhibitors (BCL2i) alone or in combination with each other or other compounds have proven superior to chemoimmunotherapy (CIT) in both the frontline and the relapsed/refractory (R/R) setting.<span><sup>1</sup></span></p><p>ERIC, the European Research Initiative on CLL, conducted this international multicenter retrospective study focused on the era of CIT, aiming to (i) reveal the treatment patterns in the “real world” and (ii) assess the outcomes of patients who received frontline treatment between 2000 and 2016. Overall, 7382 patients with CLL (7134, 96.6%) or SLL (248, 3.4%) from 76 centers in 25 countries in five continents were included. The median age at diagnosis was 64 (interquartile range [IQR]: 56–71) years and the median age at first treatment was 66 (IQR: 58–74) years. The median follow-up was 7.33 (IQR: 4.56–10.81) years from diagnosis and 5.27 (IQR: 3.04–7.99) from first treatment. The vast majority of patients (6873/7134, 93.2%) received at least one line of chemotherapy or CIT; only 197/7134 (2.7%) received exclusively novel agents. Baseline characteristics and disease-specific biomarkers are listed in Supporting Information Material.</p><p>The most common first-line regimen was FCR (2609, 35.3%), mostly in young patients (median age at first treatment: 60 years, IQR: 54–66), followed by chlorambucil monotherapy (1293, 17.5%), mostly in older patients (median age at first treatment: 74 years, IQR: 65–80). BTKis as first-line treatment were used in 149/7134 (2%) patients who either participated in clinical trials and/or had <i>TP53</i> aberrations; 20/7134 (0.3%) received frontline venetoclax-based regimens, all in the context of clinical trials (Figure 1). Detailed outcomes for the most common frontline regimens are provided in Supporting Information Material.</p><p>BTKis were the most common type of R/R treatment (1581/8145, 19.4%). Reflecting the approval of novel agents for patients with R/R CLL, the use of all types of chemotherapy and CIT decreased after 2014, except bendamustine plus rituximab (Figure 2).</p><p>There were 387 patients with an early (<24 months) need for second-line treatment after 2016: 203/387 (52.4%) received chemotherapy and CIT, 147/387 (38%) novel agents (108/387 [27.9%] BTKi, 24/387 [6.2%] PI3Ki, and 15/387 [3.9%] venetoclax-based treatments), and 37/387 (9.6%) other treatments (Figure 2 & File S1). ORR and discontinuation rates due to progression of patients treated with novel agents are given in the File S1.</p><p>Among patients treated with BTKi with or without anti-CD20 monoclonal antibodies (Mab), 55/567 (9.7%) discontinued treatment due to toxicity in second and 120/1014 (11.8%) in later lines. The median time to discontinuation was 5 months (95% confidence interval [CI]: 3.7–12.5) for patients treated in second line and 14 months (95% CI: 8–20.9) for patients treated in later line. Patients treated with BTKi in second line discontinued treatment due to toxicity earlier compared to those treated at later lines. Considering that administration of BTKi in second versus later lines happened more recently, this may simply reflect the fact that physicians had more choices and discontinued faster in second line. Taken together, our findings mirror the long-term results of the RESONATE trial yet are strikingly lower compared to the “real world” study by Mato et al.,<span><sup>2, 3</sup></span> despite the longer median follow-up on ibrutinib in our study (>27 vs. 17 months). We attribute this difference to a number of reasons. First, the aforementioned study included patients treated soon after ibrutinib approval when physicians may have been less experienced on how to manage new adverse events. Second, most patients in our study derived from large academic centers with expertise in managing patients with CLL, including ibrutinib-related toxicities. Third, differences in patients' fitness status and comorbidity burden could have influenced physician decisions. Finally, cultural and healthcare system differences between the United States and the rest of the world may have also played a role.</p><p>Patients treated with PI3Ki with or without an anti-CD20 Mab had the numerically highest toxicity-related discontinuation rates (24/76 [31.6%] and 84/285 [29.5%] in second or later line, respectively) (median time to discontinuation: 8.1 months [95% CI: 5–14.2] in second line and 10.8 [8–12] in later line), confirming the safety issues of previous studies.<span><sup>4-6</sup></span></p><p>Continuous venetoclax therapy was discontinued due to toxicity in 3/60 (5%) and 20/179 (7%) patients in second or later line, respectively (median time to discontinuation: 38.6 months [95% CI: 37.6–not estimable] in second line and 4.5 months [2.5–25] in later line). None of the 29 patients treated with BTKi plus venetoclax with or without an anti-CD20 Mab discontinued treatment due to toxicity, while only 1/56 (1.8%) (at 5.1 months after treatment initiation) and 4/112 (3.6%) discontinued venetoclax plus rituximab in second or later line, respectively (in later line, the median time to discontinuation was 4.6 months [1.6–not estimable]).</p><p>Infection was a common reason for discontinuation of all novel agent-based therapies (18/64 (28.1%), 16/60 (26.7%), and 8/15 (53.3%) for BTKi, PI3Ki, and venetoclax-based treatments, respectively). Most patients discontinued BTKi and PI3Ki-based treatments due to unspecified nonhematological toxicity (28/64 [43.8%] and 23/60 [38.3%], respectively). Atrial fibrillation/flutter (6/64, 9.4%) and autoimmune phenomena (15/60, 25%) were among the prevailing reasons for discontinuation in BTKi and PI3Ki-treated patients, respectively. Cytopenias (5/15, 33.3%) were the second most common reason (after infection) for discontinuing venetoclax-based treatments.</p><p>Information on tumor lysis syndrome (TLS) was available on 148 patients with R/R CLL treated with venetoclax-based regimens. Only 2/148 (1.4%) patients, both high-risk for TLS, developed clinical TLS; laboratory TLS was present in 8/148 (5.4%) patients. Information on the timing of TLS and the ramp-up scheme/TLS prophylaxis in each case were not captured. All patients who developed TLS recovered and continued treatment. Our results are in line with RCTs and previous large “real world” studies,<span><sup>7-13</sup></span> highlighting the ability of hematologists to prevent this adverse event in the “real-world” setting.</p><p>Seventy-one patients were double refractory to both BTKi and venetoclax (File S1). Most patients with available biomarkers had unmutated IGHV genes (34/43, 79.1%) and 64.5% (20/31) had <i>TP53</i> aberrations before first-line treatment. After the second novel agent failure, 62% (44/71) received an additional line of therapy. The median time-to-next treatment (TTNT) from the second novel agent treatment was 11.4 months (95% CI: 7.95–14.65) and the median overall survival (OS) from the second novel agent treatment was 19.88 months (95% CI: 14.72–30.32). Overall, 43 patients received a subsequent line of therapy for CLL after failing the second targeted agent. The median OS and TTNT from the start of the subsequent line of treatment were 12 and 9 months, respectively. Hence, we confirm the poor prognosis of these patients reported in previous “real world” studies, especially when noncovalent BTKis and other novel approaches (e.g., CAR-T cells) are unavailable.<span><sup>14, 15</sup></span></p><p>In a multivariable analysis in patients receiving frontline therapy, increased age, male sex, unmutated IGHV genes, and <i>TP53</i> aberrations predicted a shorter TTNT, while unmutated IGHV gene status was the only statistically significant predictor for the need for the next treatment (File S1), perhaps reflecting missing information on <i>TP53</i> mutation status in 71.3% (5266/7382) of patients. FCR conferred a longer TTNT (<i>p</i> = 0.002, 95% CI: 0.64–0.91) versus other types of frontline treatment. Similarly, in patients with R/R CLL, increased age at second-line treatment, unmutated IGHV genes, and <i>TP53</i> aberrations were statistically significant predictors for a shorter OS. The only protective factor from death in patients with R/R CLL was treatment with novel agents in the first or second line (File S1), highlighting the importance of incorporating novel agents early in the CLL treatment algorithm.</p><p>We chart a major shift in treatment patterns before and after the introduction of novel targeted agents in 2014. Against that, many patients with R/R CLL in our cohort were still treated with CIT even after 2014. This may be explained, at least in part, by the fact that CIT was considered a valid retreatment option for patients with long first remissions for quite some time after 2014. Notably, even after 2016, novel agents were used in only 38% of patients with an early (<24 months) need for second-line treatment. Possible reasons include access to medication, physicians' reluctance, and the evidence–practice gap. This highlights the need for more timely and effective knowledge dissemination, but even more importantly, reduction of drug costs and adoption of less strict rules for drug reimbursement.</p><p>We acknowledge certain limitations to our study. First, the median age at diagnosis and first treatment is lower than traditionally expected, perhaps due to the fact that many patients were included from referral centers for CLL. Second, the assessment of response was performed by treating physicians based mainly on complete blood counts and physical examination, likely overestimating the response in some cases. Finally, missing information, sampling, and attrition bias also apply. Recognizing these limitations, we mitigated them by collecting data on consecutively treated patients in each participating center and focusing on robust metrics (i.e., TTNT and OS).</p><p>Altogether, we document the effectiveness and safety of novel agents in patients with R/R CLL previously treated with CIT or chemotherapy regimens. We also witness a great delay in the timely implementation of the existing evidence in the real world with a slow uptake of drugs proven to be highly efficacious. Thus, dedicated efforts to improve it should be considered for the future generation of treatments.</p><p>Thomas Chatzikonstantinou and Lydia Scarfò collected data, coordinated the study, wrote the paper, assessed and verified the data, and performed the analysis. Georgios Karakatsoulis wrote the paper and performed the analysis. Gloria Iacoboni, Jana Kotaskova, and CD collected data, coordinated the study, and contributed to interpretation and manuscript editing. Eva Minga and Dimitra Chamou coordinated the data collection, curate the data, and contributed to interpretation and manuscript editing. Elisa Albi, Miguel Alcoceba, Salem Al-Shemari, Thérèse Aurran-Schleinitz, Francesca Bacchiarri, Sofia Chatzileontiadou, Rosa Collado, Zadie Davis, Marcos Daniel de Deus Santos, Maria Dimou, Elena Dmitrieva, David Donaldson, Gimena Dos Santos, Barbara Dreta, Maria Efstathopoulou, Shaimaa El-Ashwah, Alicia Enrico, Andrzej Frygier, Sara Galimberti, Andrea Galitzia, Eva Gimeno, Valerio Guarente, Romain Guieze, Sean Harrop, Eleftheria Hatzimichael, Yair Herishanu, José-Ángel Hernández-Rivas, Ozren Jaksic, Elżbieta Kalicińska, Kamel Laribi, Volkan Karakus, Arnon P. Kater, Bonnie Kho, Maria Kislova, Εliana Konstantinou, Maya Koren-Michowitz, Ioannis Kotsianidis, Zuzana Kubova, Jorge Labrador, Deepesh Lad, Luca Laurenti, Thomas Longval, Alberto Lopez-Garcia, Juan Marquet, Stanislava Maslejova, Carlota Mayor-Bastida, Biljana Mihaljevic, Ivana Milosevic, Fatima Miras, Riccardo Moia, Marta Morawska, Uttam K. Nath, Almudena Navarro-Bailón, Jacopo Olivieri, Irina Panovska-Stavridis, Maria Papaioannou, Cheyenne Pierie, Anna Puiggros, Gianluigi Reda, Gian Matteo Rigolin, Rosa Ruchlemer, Mattia Schipani, Annett Schiwitza, Yandong Shen, Tereza Shokralla, Martin Simkovic, Svetlana Smirnova, Dina S. A. Soliman, Stephan Stilgenbauer, Tamar Tadmor, Kristina Tomic, Eric Tse, Theodoros Vassilakopoulos, Andrea Visentin, Candida Vitale, George Vrachiolias, Vojin Vukovic, Renata Walewska, Zhenshu Xu, Munci Yagci, Lucrecia Yañez, Mohamed Yassin, Jana Zuchnicka, David Oscier, Alessandro Gozzetti, Panagiotis Panagiotidis, Francesc Bosch, Blanca Espinet, Paolo Sportoletti, Gerassimos A. Pangalis, Viola M. Popov, Stephen Mulligan, Maria Angelopoulou, Fatih Demirkan, Tomas Papajík, Bella Biderman, Roberta Murru, Marta Coscia, Constantine Tam, Antonio Cuneo, Gianluca Gaidano, Rainer Claus, Niki Stavroyianni, Livio Trentin, Darko Antic, Lukas Smolej, Olga B. Kalashnikova, Mark Catherwood, Martin Spacek, Sarka Pospisilova, Michael Doubek, Eugene Nikitin, and Anastasia Chatzidimitriou collected data and contributed to interpretation and manuscript editing. Paolo Ghia and Kostas Stamatopoulos designed and coordinated the study and wrote the paper.</p><p>Thomas Chatzikonstantinou received honoraria from AbbVie. Lydia Scarfò received honoraria from AbbVie, AstraZeneca, BeiGene, Lilly, Janssen, Octapharma. Gloria Iacoboni received honoraria and travel support from Novartis, Kite/Gilead, Bristol-Myers Squibb, Abbvie, Autolus, Miltenyi, and AstraZeneca. Rosa Collado received support for attending meetings from Janssen-Cilag and S.A. Sara Galimberti received honoraria support for attending meetings from AbbVie, AstraZeneca, Jazz, Novartis, and Incyte, honoraria from Roche, Celgene, Pfizer, and Janssen, and support for attending meetings from Jazz, AstraZeneca, and Roche. Romain Guieze received honoraria, consulting fees, and support for attending meetings from AbbVie, Beigene, Roche, Janssen, and AstraZeneca. Eleftheria Hatzimichael received honoraria from AbbVie, Janssen-Cilag, AstraZeneca, and Roche. Yair Herishanu received honoraria from Janssen, AbbVie, Roche, AstraZeneca, Medion, and Lilly. José-Ángel Hernández-Rivas received honoraria as a consultant from Janssen, AbbVie, AstraZeneca, Lilly, and BeiGene and support for attending meetings from Janssen, AbbVie, AstraZeneca, and BeiGene. Ozren Jaksic received honoraria from Johnson and Johnson, AstraZeneca, and Lilly, honoraria from Johnson and Johnson, AbbVie, AstraZeneca, and Lilly, and support for attending meetings from Johnson and Johnson, and AbbVie. Kamel Laribi received consulting fees from AbbVie, AstraZeneca, Janssen, Beigene, Takeda, and Novartis. Maya Koren-Michowitz received honoraria from Novartis, Pfizer, and Gad Medical LTD. and support for attending meetings from Novartis. Arnon P. Kater received advisory board fees and research money from Janssen, AbbVie, BMS, AstraZeneca, and Roche/Genentech, and support for attending meetings from Janssen and AbbVie. Ioannis Kotsianidis received honoraria and consulting fees from AbbVie and Janssen. Ivana Milosevic received honoraria from AbbVie, Roche, Sandoz, AstraZeneca, and Janssen, and support for attending meetings from AbbVie, Roche, and Takeda. Almudena Navarro-Bailón received honoraria, advisory board fees, and support for attending meetings from AbbVie, AstraZeneca, Takeda, Janssen, and Beigene. Jacopo Olivieri received honoraria from AbbVie, AstraZeneca, and Janssen. Gianluigi Reda received consulting fees from AbbVie, AstraZeneca, Janssen, and Beigene, and is currently employed by AstraZeneca. Gian M. Rigolin received honoraria for participation in speaker's bureau from AbbVie, Astra Zeneca, Beigene, and Janssen, and support for attending meetings from Janssen. Mattia Schipani received honoraria and support for attending meetings from AstraZeneca, AbbVie, and Janssen-Cilag and owns shares of stock in AbbVie, AstraZeneca, Merck, Eli Lilly, Sanofi, Johnson and Johnson, Pfizer, Gilead, and GSK. Tereza Shokralla and Stephan Stilgenbauer reports research funding from, consultancy or advisory role for, honoraria from, speakers' bureau participation for, and travel support from AbbVie, Amgen, AstraZeneca, BeiGene, Bristol Myers Squibb, Celgene, Gilead, GlaxoSmithKline, Hoffmann-La Roche, Incyte, Infinity, Janssen, Novartis, and Sunesis. Eric Tse received support for attending meetings from Takeda. Theodoros Vassilakopoulos received honoraria from Takeda, Roche, Genesis Pharma, Merck, Novartis, Gilead, Sandoz, AstraZeneca, Integris, and Servier, and support for attending meetings from Takeda, Roche, Genesis Pharma, Merck, Pfizer, and Winmedica. Candida Vitale received honoraria from AbbVie, consulting fees from AstraZeneca, and support for attending meetings from AstraZeneca, Takeda, and Janssen. Renata Walewska received honoraria from AbbVie, AstraZeneca, and Beigene, support for attending meetings from Janssen, AbbVie, and AstraZeneca, and advisory board fees from AbbVie, AstraZeneca, Janssen, Beigene, and SecuraBio. Lucrecia Yañez received honoraria from AbbVie, AstraZeneca, Novartis, Gilead, Janssen, Jazz, MSD, and Pfizer, support for attending meetings from AbbVie, AstraZeneca, Gilead, Janssen, and Pfizer, and advisory board fees from AbbVie, AstraZeneca, Jazz, Janssen, Beigene, and Celgene. Francesc Bosch received consulting fees, honoraria, and payment for expert testimony from AbbVie, Genentech, Novartis, Takeda, Janssen, Roche, Mundipharma, Celgene/BMS, AstraZeneca, Lilly, Beigene, Gilead and TG Therapeutics, Advantage Allogene, Lava Therapeutics, and Enterome. Stephen Mulligan received advisory board fees from AbbVie, AstraZeneca, Janssen, Roche, and BeiGene. Maria Angelopoulou received consulting fees from AbbVie, Takeda, Janssen, Roche, Genesis, Gilead, and Amgen and honoraria from AbbVie, Takeda, Roche, Genesis, Gilead, and Novartis. Fatih Demirkan received support for attending meetings from Janssen and AbbVie. Tomas Papajík received honoraria and advisory board fees from AbbVie, Janssen-Cilag, and AstraZeneca, and support for attending meetings from AstraZeneca. Marta Coscia received honoraria, advisory board fees, and support for attending meetings from AbbVie, AstraZeneca, and Janssen. Constantine Tam received honoraria from AbbVie, Beigene, Janssen, and LOXO. Antonio Cuneo received honoraria, advisory board fees, and support for attending meetings from AbbVie, AstraZeneca, Beigene, Janssen, and Lilly. Gianluca Gaidano received honoraria from Abbvie, AstraZeneca, BeiGene, Hikma, Incyte, Janssen, and Lilly. Niki Stavroyianni received honoraria from Janssen, AbbVie, AstraZeneca, and Lilly, and support for attending meetings from Janssen and AstraZeneca. Lukas Smolej received consulting fees, honoraria, and support for attending meetings from AbbVie, AstraZeneca, and Janssen and advisory board fees from AbbVie and AstraZeneca. Martin Spacek received honoraria and consulting and advisory board fees, and support for attending meetings from AbbVie, AstraZeneca, and Janssen. Michael Doubek received research support and honoraria from AbbVie, AstraZeneca, and Janssen. Eugene Nikitin received honoraria from AbbVie. Kostas Stamatopoulos received research support from AbbVie, AstraZeneca, Janssen, Novartis, and Roche; honoraria from AbbVie, AstraZeneca, Bristol Myers Squibb, Lilly, and Janssen. Paolo Ghia received research support from AbbVie, AstraZeneca, BMS, Janssen and honoraria from AbbVie, AstraZeneca, BeiGene, BMS, Galapagos, Genmab, Janssen, Loxo Oncology @Lilly, MSD, Roche, and is an Editor of HemaSphere.</p><p>Georgios Karakatsoulis, Eva Minga, Dimitra Chamou, Jana Kotaskova, Christos Demosthenous, Elisa Albi, Miguel Alcoceba, Salem Al-Shemari, Thérèse Aurran-Schleinitz, Francesca Bacchiarri, Sofia Chatzileontiadou, Zadie Davis, Marcos Daniel de Deus Santos, Maria Dimou, Elena Dmitrieva, David Donaldson, Gimena Dos Santos, Barbara Dreta, Maria Efstathopoulou, Shaimaa El-Ashwah, Alicia Enrico, Andrzej Frygier, Andrea Galitzia, Eva Gimeno, Valerio Guarente, Sean Harrop, Elżbieta Kalicińska, Volkan Karakus, Bonnie Kho, Maria Kislova, Εliana Konstantinou, Zuzana Kubova, Jorge Labrador, Deepesh Lad, Luca Laurenti, Thomas Longval, Alberto Lopez-Garcia, Juan Marquet, Stanislava Maslejova, Carlota Mayor-Bastida, Biljana Mihaljevic, Fatima Miras, Riccardo Moia, Marta Morawska, Uttam K. Nath, Irina Panovska-Stavridis, Maria Papaioannou, Cheyenne Pierie, Anna Puiggros, Rosa Ruchlemer, Annett Schiwitza, Yandong Shen, Tereza Shokralla, Martin Simkovic, Svetlana Smirnova, Dina S. A. Soliman, Tamar Tadmor, Kristina Tomic, Andrea Visentin, George Vrachiolias, Vojin Vukovic, Zhenshu Xu, Munci Yagci, Mohamed Yassin, Jana Zuchnicka, David Oscier, Alessandro Gozzetti, Panagiotis Panagiotidis, Blanca Espinet, Paolo Sportoletti, Gerassimos A. Pangalis, Viola M. Popov, Bella Biderman, Roberta Murru, Rainer Claus, Livio Trentin, Darko Antic, Olga B. Kalashnikova, Mark Catherwood, Sarka Pospisilova, and Anastasia Chatzidimitriou have no conflict of interest to disclose.</p><p>This project was supported in part by AbbVie; AIRC under 5 per Mille 2018-ID. 21198 program (to PG and GG); PNRR-MAD-2022-12375673 (Next Generation EU, M6/C2_CALL 2022), Italian Ministry of Health, Rome, Italy, Conceptual development of research organization (FNBr 65269705) provided by the Ministry of Health of the Czech Republic, and National Institute for Cancer Research (Programme EXCELLES, ID Project No. LX22NPO5102) funded by the European Union—Next Generation EU.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 9","pages":""},"PeriodicalIF":14.6000,"publicationDate":"2024-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.70004","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.70004","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Novel small molecule inhibitors have revolutionized the treatment of chronic lymphocytic leukemia (CLL). Indeed, BTK (BTKi) and BCL2 inhibitors (BCL2i) alone or in combination with each other or other compounds have proven superior to chemoimmunotherapy (CIT) in both the frontline and the relapsed/refractory (R/R) setting.1
ERIC, the European Research Initiative on CLL, conducted this international multicenter retrospective study focused on the era of CIT, aiming to (i) reveal the treatment patterns in the “real world” and (ii) assess the outcomes of patients who received frontline treatment between 2000 and 2016. Overall, 7382 patients with CLL (7134, 96.6%) or SLL (248, 3.4%) from 76 centers in 25 countries in five continents were included. The median age at diagnosis was 64 (interquartile range [IQR]: 56–71) years and the median age at first treatment was 66 (IQR: 58–74) years. The median follow-up was 7.33 (IQR: 4.56–10.81) years from diagnosis and 5.27 (IQR: 3.04–7.99) from first treatment. The vast majority of patients (6873/7134, 93.2%) received at least one line of chemotherapy or CIT; only 197/7134 (2.7%) received exclusively novel agents. Baseline characteristics and disease-specific biomarkers are listed in Supporting Information Material.
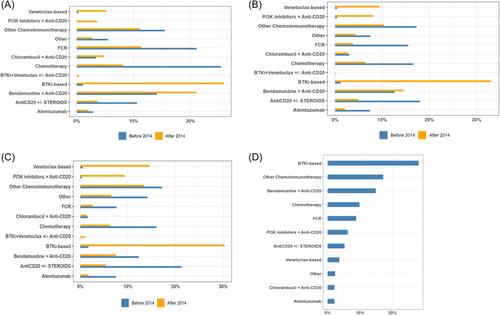
The most common first-line regimen was FCR (2609, 35.3%), mostly in young patients (median age at first treatment: 60 years, IQR: 54–66), followed by chlorambucil monotherapy (1293, 17.5%), mostly in older patients (median age at first treatment: 74 years, IQR: 65–80). BTKis as first-line treatment were used in 149/7134 (2%) patients who either participated in clinical trials and/or had TP53 aberrations; 20/7134 (0.3%) received frontline venetoclax-based regimens, all in the context of clinical trials (Figure 1). Detailed outcomes for the most common frontline regimens are provided in Supporting Information Material.
BTKis were the most common type of R/R treatment (1581/8145, 19.4%). Reflecting the approval of novel agents for patients with R/R CLL, the use of all types of chemotherapy and CIT decreased after 2014, except bendamustine plus rituximab (Figure 2).
There were 387 patients with an early (<24 months) need for second-line treatment after 2016: 203/387 (52.4%) received chemotherapy and CIT, 147/387 (38%) novel agents (108/387 [27.9%] BTKi, 24/387 [6.2%] PI3Ki, and 15/387 [3.9%] venetoclax-based treatments), and 37/387 (9.6%) other treatments (Figure 2 & File S1). ORR and discontinuation rates due to progression of patients treated with novel agents are given in the File S1.
Among patients treated with BTKi with or without anti-CD20 monoclonal antibodies (Mab), 55/567 (9.7%) discontinued treatment due to toxicity in second and 120/1014 (11.8%) in later lines. The median time to discontinuation was 5 months (95% confidence interval [CI]: 3.7–12.5) for patients treated in second line and 14 months (95% CI: 8–20.9) for patients treated in later line. Patients treated with BTKi in second line discontinued treatment due to toxicity earlier compared to those treated at later lines. Considering that administration of BTKi in second versus later lines happened more recently, this may simply reflect the fact that physicians had more choices and discontinued faster in second line. Taken together, our findings mirror the long-term results of the RESONATE trial yet are strikingly lower compared to the “real world” study by Mato et al.,2, 3 despite the longer median follow-up on ibrutinib in our study (>27 vs. 17 months). We attribute this difference to a number of reasons. First, the aforementioned study included patients treated soon after ibrutinib approval when physicians may have been less experienced on how to manage new adverse events. Second, most patients in our study derived from large academic centers with expertise in managing patients with CLL, including ibrutinib-related toxicities. Third, differences in patients' fitness status and comorbidity burden could have influenced physician decisions. Finally, cultural and healthcare system differences between the United States and the rest of the world may have also played a role.
Patients treated with PI3Ki with or without an anti-CD20 Mab had the numerically highest toxicity-related discontinuation rates (24/76 [31.6%] and 84/285 [29.5%] in second or later line, respectively) (median time to discontinuation: 8.1 months [95% CI: 5–14.2] in second line and 10.8 [8–12] in later line), confirming the safety issues of previous studies.4-6
Continuous venetoclax therapy was discontinued due to toxicity in 3/60 (5%) and 20/179 (7%) patients in second or later line, respectively (median time to discontinuation: 38.6 months [95% CI: 37.6–not estimable] in second line and 4.5 months [2.5–25] in later line). None of the 29 patients treated with BTKi plus venetoclax with or without an anti-CD20 Mab discontinued treatment due to toxicity, while only 1/56 (1.8%) (at 5.1 months after treatment initiation) and 4/112 (3.6%) discontinued venetoclax plus rituximab in second or later line, respectively (in later line, the median time to discontinuation was 4.6 months [1.6–not estimable]).
Infection was a common reason for discontinuation of all novel agent-based therapies (18/64 (28.1%), 16/60 (26.7%), and 8/15 (53.3%) for BTKi, PI3Ki, and venetoclax-based treatments, respectively). Most patients discontinued BTKi and PI3Ki-based treatments due to unspecified nonhematological toxicity (28/64 [43.8%] and 23/60 [38.3%], respectively). Atrial fibrillation/flutter (6/64, 9.4%) and autoimmune phenomena (15/60, 25%) were among the prevailing reasons for discontinuation in BTKi and PI3Ki-treated patients, respectively. Cytopenias (5/15, 33.3%) were the second most common reason (after infection) for discontinuing venetoclax-based treatments.
Information on tumor lysis syndrome (TLS) was available on 148 patients with R/R CLL treated with venetoclax-based regimens. Only 2/148 (1.4%) patients, both high-risk for TLS, developed clinical TLS; laboratory TLS was present in 8/148 (5.4%) patients. Information on the timing of TLS and the ramp-up scheme/TLS prophylaxis in each case were not captured. All patients who developed TLS recovered and continued treatment. Our results are in line with RCTs and previous large “real world” studies,7-13 highlighting the ability of hematologists to prevent this adverse event in the “real-world” setting.
Seventy-one patients were double refractory to both BTKi and venetoclax (File S1). Most patients with available biomarkers had unmutated IGHV genes (34/43, 79.1%) and 64.5% (20/31) had TP53 aberrations before first-line treatment. After the second novel agent failure, 62% (44/71) received an additional line of therapy. The median time-to-next treatment (TTNT) from the second novel agent treatment was 11.4 months (95% CI: 7.95–14.65) and the median overall survival (OS) from the second novel agent treatment was 19.88 months (95% CI: 14.72–30.32). Overall, 43 patients received a subsequent line of therapy for CLL after failing the second targeted agent. The median OS and TTNT from the start of the subsequent line of treatment were 12 and 9 months, respectively. Hence, we confirm the poor prognosis of these patients reported in previous “real world” studies, especially when noncovalent BTKis and other novel approaches (e.g., CAR-T cells) are unavailable.14, 15
In a multivariable analysis in patients receiving frontline therapy, increased age, male sex, unmutated IGHV genes, and TP53 aberrations predicted a shorter TTNT, while unmutated IGHV gene status was the only statistically significant predictor for the need for the next treatment (File S1), perhaps reflecting missing information on TP53 mutation status in 71.3% (5266/7382) of patients. FCR conferred a longer TTNT (p = 0.002, 95% CI: 0.64–0.91) versus other types of frontline treatment. Similarly, in patients with R/R CLL, increased age at second-line treatment, unmutated IGHV genes, and TP53 aberrations were statistically significant predictors for a shorter OS. The only protective factor from death in patients with R/R CLL was treatment with novel agents in the first or second line (File S1), highlighting the importance of incorporating novel agents early in the CLL treatment algorithm.
We chart a major shift in treatment patterns before and after the introduction of novel targeted agents in 2014. Against that, many patients with R/R CLL in our cohort were still treated with CIT even after 2014. This may be explained, at least in part, by the fact that CIT was considered a valid retreatment option for patients with long first remissions for quite some time after 2014. Notably, even after 2016, novel agents were used in only 38% of patients with an early (<24 months) need for second-line treatment. Possible reasons include access to medication, physicians' reluctance, and the evidence–practice gap. This highlights the need for more timely and effective knowledge dissemination, but even more importantly, reduction of drug costs and adoption of less strict rules for drug reimbursement.
We acknowledge certain limitations to our study. First, the median age at diagnosis and first treatment is lower than traditionally expected, perhaps due to the fact that many patients were included from referral centers for CLL. Second, the assessment of response was performed by treating physicians based mainly on complete blood counts and physical examination, likely overestimating the response in some cases. Finally, missing information, sampling, and attrition bias also apply. Recognizing these limitations, we mitigated them by collecting data on consecutively treated patients in each participating center and focusing on robust metrics (i.e., TTNT and OS).
Altogether, we document the effectiveness and safety of novel agents in patients with R/R CLL previously treated with CIT or chemotherapy regimens. We also witness a great delay in the timely implementation of the existing evidence in the real world with a slow uptake of drugs proven to be highly efficacious. Thus, dedicated efforts to improve it should be considered for the future generation of treatments.
Thomas Chatzikonstantinou and Lydia Scarfò collected data, coordinated the study, wrote the paper, assessed and verified the data, and performed the analysis. Georgios Karakatsoulis wrote the paper and performed the analysis. Gloria Iacoboni, Jana Kotaskova, and CD collected data, coordinated the study, and contributed to interpretation and manuscript editing. Eva Minga and Dimitra Chamou coordinated the data collection, curate the data, and contributed to interpretation and manuscript editing. Elisa Albi, Miguel Alcoceba, Salem Al-Shemari, Thérèse Aurran-Schleinitz, Francesca Bacchiarri, Sofia Chatzileontiadou, Rosa Collado, Zadie Davis, Marcos Daniel de Deus Santos, Maria Dimou, Elena Dmitrieva, David Donaldson, Gimena Dos Santos, Barbara Dreta, Maria Efstathopoulou, Shaimaa El-Ashwah, Alicia Enrico, Andrzej Frygier, Sara Galimberti, Andrea Galitzia, Eva Gimeno, Valerio Guarente, Romain Guieze, Sean Harrop, Eleftheria Hatzimichael, Yair Herishanu, José-Ángel Hernández-Rivas, Ozren Jaksic, Elżbieta Kalicińska, Kamel Laribi, Volkan Karakus, Arnon P. Kater, Bonnie Kho, Maria Kislova, Εliana Konstantinou, Maya Koren-Michowitz, Ioannis Kotsianidis, Zuzana Kubova, Jorge Labrador, Deepesh Lad, Luca Laurenti, Thomas Longval, Alberto Lopez-Garcia, Juan Marquet, Stanislava Maslejova, Carlota Mayor-Bastida, Biljana Mihaljevic, Ivana Milosevic, Fatima Miras, Riccardo Moia, Marta Morawska, Uttam K. Nath, Almudena Navarro-Bailón, Jacopo Olivieri, Irina Panovska-Stavridis, Maria Papaioannou, Cheyenne Pierie, Anna Puiggros, Gianluigi Reda, Gian Matteo Rigolin, Rosa Ruchlemer, Mattia Schipani, Annett Schiwitza, Yandong Shen, Tereza Shokralla, Martin Simkovic, Svetlana Smirnova, Dina S. A. Soliman, Stephan Stilgenbauer, Tamar Tadmor, Kristina Tomic, Eric Tse, Theodoros Vassilakopoulos, Andrea Visentin, Candida Vitale, George Vrachiolias, Vojin Vukovic, Renata Walewska, Zhenshu Xu, Munci Yagci, Lucrecia Yañez, Mohamed Yassin, Jana Zuchnicka, David Oscier, Alessandro Gozzetti, Panagiotis Panagiotidis, Francesc Bosch, Blanca Espinet, Paolo Sportoletti, Gerassimos A. Pangalis, Viola M. Popov, Stephen Mulligan, Maria Angelopoulou, Fatih Demirkan, Tomas Papajík, Bella Biderman, Roberta Murru, Marta Coscia, Constantine Tam, Antonio Cuneo, Gianluca Gaidano, Rainer Claus, Niki Stavroyianni, Livio Trentin, Darko Antic, Lukas Smolej, Olga B. Kalashnikova, Mark Catherwood, Martin Spacek, Sarka Pospisilova, Michael Doubek, Eugene Nikitin, and Anastasia Chatzidimitriou collected data and contributed to interpretation and manuscript editing. Paolo Ghia and Kostas Stamatopoulos designed and coordinated the study and wrote the paper.
Thomas Chatzikonstantinou received honoraria from AbbVie. Lydia Scarfò received honoraria from AbbVie, AstraZeneca, BeiGene, Lilly, Janssen, Octapharma. Gloria Iacoboni received honoraria and travel support from Novartis, Kite/Gilead, Bristol-Myers Squibb, Abbvie, Autolus, Miltenyi, and AstraZeneca. Rosa Collado received support for attending meetings from Janssen-Cilag and S.A. Sara Galimberti received honoraria support for attending meetings from AbbVie, AstraZeneca, Jazz, Novartis, and Incyte, honoraria from Roche, Celgene, Pfizer, and Janssen, and support for attending meetings from Jazz, AstraZeneca, and Roche. Romain Guieze received honoraria, consulting fees, and support for attending meetings from AbbVie, Beigene, Roche, Janssen, and AstraZeneca. Eleftheria Hatzimichael received honoraria from AbbVie, Janssen-Cilag, AstraZeneca, and Roche. Yair Herishanu received honoraria from Janssen, AbbVie, Roche, AstraZeneca, Medion, and Lilly. José-Ángel Hernández-Rivas received honoraria as a consultant from Janssen, AbbVie, AstraZeneca, Lilly, and BeiGene and support for attending meetings from Janssen, AbbVie, AstraZeneca, and BeiGene. Ozren Jaksic received honoraria from Johnson and Johnson, AstraZeneca, and Lilly, honoraria from Johnson and Johnson, AbbVie, AstraZeneca, and Lilly, and support for attending meetings from Johnson and Johnson, and AbbVie. Kamel Laribi received consulting fees from AbbVie, AstraZeneca, Janssen, Beigene, Takeda, and Novartis. Maya Koren-Michowitz received honoraria from Novartis, Pfizer, and Gad Medical LTD. and support for attending meetings from Novartis. Arnon P. Kater received advisory board fees and research money from Janssen, AbbVie, BMS, AstraZeneca, and Roche/Genentech, and support for attending meetings from Janssen and AbbVie. Ioannis Kotsianidis received honoraria and consulting fees from AbbVie and Janssen. Ivana Milosevic received honoraria from AbbVie, Roche, Sandoz, AstraZeneca, and Janssen, and support for attending meetings from AbbVie, Roche, and Takeda. Almudena Navarro-Bailón received honoraria, advisory board fees, and support for attending meetings from AbbVie, AstraZeneca, Takeda, Janssen, and Beigene. Jacopo Olivieri received honoraria from AbbVie, AstraZeneca, and Janssen. Gianluigi Reda received consulting fees from AbbVie, AstraZeneca, Janssen, and Beigene, and is currently employed by AstraZeneca. Gian M. Rigolin received honoraria for participation in speaker's bureau from AbbVie, Astra Zeneca, Beigene, and Janssen, and support for attending meetings from Janssen. Mattia Schipani received honoraria and support for attending meetings from AstraZeneca, AbbVie, and Janssen-Cilag and owns shares of stock in AbbVie, AstraZeneca, Merck, Eli Lilly, Sanofi, Johnson and Johnson, Pfizer, Gilead, and GSK. Tereza Shokralla and Stephan Stilgenbauer reports research funding from, consultancy or advisory role for, honoraria from, speakers' bureau participation for, and travel support from AbbVie, Amgen, AstraZeneca, BeiGene, Bristol Myers Squibb, Celgene, Gilead, GlaxoSmithKline, Hoffmann-La Roche, Incyte, Infinity, Janssen, Novartis, and Sunesis. Eric Tse received support for attending meetings from Takeda. Theodoros Vassilakopoulos received honoraria from Takeda, Roche, Genesis Pharma, Merck, Novartis, Gilead, Sandoz, AstraZeneca, Integris, and Servier, and support for attending meetings from Takeda, Roche, Genesis Pharma, Merck, Pfizer, and Winmedica. Candida Vitale received honoraria from AbbVie, consulting fees from AstraZeneca, and support for attending meetings from AstraZeneca, Takeda, and Janssen. Renata Walewska received honoraria from AbbVie, AstraZeneca, and Beigene, support for attending meetings from Janssen, AbbVie, and AstraZeneca, and advisory board fees from AbbVie, AstraZeneca, Janssen, Beigene, and SecuraBio. Lucrecia Yañez received honoraria from AbbVie, AstraZeneca, Novartis, Gilead, Janssen, Jazz, MSD, and Pfizer, support for attending meetings from AbbVie, AstraZeneca, Gilead, Janssen, and Pfizer, and advisory board fees from AbbVie, AstraZeneca, Jazz, Janssen, Beigene, and Celgene. Francesc Bosch received consulting fees, honoraria, and payment for expert testimony from AbbVie, Genentech, Novartis, Takeda, Janssen, Roche, Mundipharma, Celgene/BMS, AstraZeneca, Lilly, Beigene, Gilead and TG Therapeutics, Advantage Allogene, Lava Therapeutics, and Enterome. Stephen Mulligan received advisory board fees from AbbVie, AstraZeneca, Janssen, Roche, and BeiGene. Maria Angelopoulou received consulting fees from AbbVie, Takeda, Janssen, Roche, Genesis, Gilead, and Amgen and honoraria from AbbVie, Takeda, Roche, Genesis, Gilead, and Novartis. Fatih Demirkan received support for attending meetings from Janssen and AbbVie. Tomas Papajík received honoraria and advisory board fees from AbbVie, Janssen-Cilag, and AstraZeneca, and support for attending meetings from AstraZeneca. Marta Coscia received honoraria, advisory board fees, and support for attending meetings from AbbVie, AstraZeneca, and Janssen. Constantine Tam received honoraria from AbbVie, Beigene, Janssen, and LOXO. Antonio Cuneo received honoraria, advisory board fees, and support for attending meetings from AbbVie, AstraZeneca, Beigene, Janssen, and Lilly. Gianluca Gaidano received honoraria from Abbvie, AstraZeneca, BeiGene, Hikma, Incyte, Janssen, and Lilly. Niki Stavroyianni received honoraria from Janssen, AbbVie, AstraZeneca, and Lilly, and support for attending meetings from Janssen and AstraZeneca. Lukas Smolej received consulting fees, honoraria, and support for attending meetings from AbbVie, AstraZeneca, and Janssen and advisory board fees from AbbVie and AstraZeneca. Martin Spacek received honoraria and consulting and advisory board fees, and support for attending meetings from AbbVie, AstraZeneca, and Janssen. Michael Doubek received research support and honoraria from AbbVie, AstraZeneca, and Janssen. Eugene Nikitin received honoraria from AbbVie. Kostas Stamatopoulos received research support from AbbVie, AstraZeneca, Janssen, Novartis, and Roche; honoraria from AbbVie, AstraZeneca, Bristol Myers Squibb, Lilly, and Janssen. Paolo Ghia received research support from AbbVie, AstraZeneca, BMS, Janssen and honoraria from AbbVie, AstraZeneca, BeiGene, BMS, Galapagos, Genmab, Janssen, Loxo Oncology @Lilly, MSD, Roche, and is an Editor of HemaSphere.
Georgios Karakatsoulis, Eva Minga, Dimitra Chamou, Jana Kotaskova, Christos Demosthenous, Elisa Albi, Miguel Alcoceba, Salem Al-Shemari, Thérèse Aurran-Schleinitz, Francesca Bacchiarri, Sofia Chatzileontiadou, Zadie Davis, Marcos Daniel de Deus Santos, Maria Dimou, Elena Dmitrieva, David Donaldson, Gimena Dos Santos, Barbara Dreta, Maria Efstathopoulou, Shaimaa El-Ashwah, Alicia Enrico, Andrzej Frygier, Andrea Galitzia, Eva Gimeno, Valerio Guarente, Sean Harrop, Elżbieta Kalicińska, Volkan Karakus, Bonnie Kho, Maria Kislova, Εliana Konstantinou, Zuzana Kubova, Jorge Labrador, Deepesh Lad, Luca Laurenti, Thomas Longval, Alberto Lopez-Garcia, Juan Marquet, Stanislava Maslejova, Carlota Mayor-Bastida, Biljana Mihaljevic, Fatima Miras, Riccardo Moia, Marta Morawska, Uttam K. Nath, Irina Panovska-Stavridis, Maria Papaioannou, Cheyenne Pierie, Anna Puiggros, Rosa Ruchlemer, Annett Schiwitza, Yandong Shen, Tereza Shokralla, Martin Simkovic, Svetlana Smirnova, Dina S. A. Soliman, Tamar Tadmor, Kristina Tomic, Andrea Visentin, George Vrachiolias, Vojin Vukovic, Zhenshu Xu, Munci Yagci, Mohamed Yassin, Jana Zuchnicka, David Oscier, Alessandro Gozzetti, Panagiotis Panagiotidis, Blanca Espinet, Paolo Sportoletti, Gerassimos A. Pangalis, Viola M. Popov, Bella Biderman, Roberta Murru, Rainer Claus, Livio Trentin, Darko Antic, Olga B. Kalashnikova, Mark Catherwood, Sarka Pospisilova, and Anastasia Chatzidimitriou have no conflict of interest to disclose.
This project was supported in part by AbbVie; AIRC under 5 per Mille 2018-ID. 21198 program (to PG and GG); PNRR-MAD-2022-12375673 (Next Generation EU, M6/C2_CALL 2022), Italian Ministry of Health, Rome, Italy, Conceptual development of research organization (FNBr 65269705) provided by the Ministry of Health of the Czech Republic, and National Institute for Cancer Research (Programme EXCELLES, ID Project No. LX22NPO5102) funded by the European Union—Next Generation EU.
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
