{"title":"Chest wall muscle area, ventilatory efficiency and exercise capacity in systemic sclerosis","authors":"Nicola Galea, Amalia Colalillo, Serena Paciulli, Chiara Pellicano, Martina Giannetti, Emanuele Possente, Gregorino Paone, Antonella Romaniello, Maurizio Muscaritoli, Edoardo Rosato, Antonietta Gigante","doi":"10.1007/s11739-024-03751-z","DOIUrl":null,"url":null,"abstract":"<p>To investigate the potential contribution of chest wall muscle area (CWMA) to the ventilatory efficiency and exercise capacity in patients with Systemic Sclerosis (SSc) without interstitial lung disease (ILD). Forty-four consecutive SSc patients [<i>F</i> = 37, median age 53.5 years (IQR 43.5–58)] were examined using chest high-resolution computed tomography (HRCT), pulmonary function tests and cardiopulmonary exercise testing (CPET). The CWMA was evaluated at the level of the ninth thoracic vertebra on CT images by two independent evaluators blinded to the patient information. CPET parameters analyzed were maximum oxygen uptake (VO2 max) and VO2 at anaerobic threshold (VO<sub>2</sub>@AT); minute ventilation (VE); maximum tidal volume (VT). A statistically significant positive correlation was found between CWMA and maximum workload (r = 0.470, <i>p</i> < 0.01), VO2 max ml/min (<i>r</i> = 0.380, <i>p</i> < 0.01), VO2@AT (<i>r</i> = 0.343, <i>p</i> < 0.05), VE (<i>r</i> = 0.308, <i>p</i> < 0.05), VT (<i>r</i> = 0.410, <i>p</i> < 0.01) and VO2/heart rate (<i>r</i> = 0.399, <i>p</i> < 0.01). In multiple regression analysis, VO2 max (ml/min) was significantly associated with CWMA [<i>β</i> coefficient = 5.226 (95% CI 2.824, 7.628); <i>p</i> < 0.001], diffusing capacity for carbon monoxide (DLco) [<i>β</i> coefficient = 6.749 (95% CI 1.460, 12.039); <i>p</i> < 0.05] and body mass index (BMI) [<i>β</i> coefficient = 41.481 (95% CI 8.802, 74.161); <i>p</i> < 0.05]. In multiple regression analysis, maximum workload was significantly associated with CWMA [<i>β</i> coefficient = 0.490 (95% CI 0.289, 0.691); <i>p</i> < 0.001], DLco [<i>β</i> coefficient = 0.645 (95% CI 0.202, 1.088); <i>p</i> < 0.01] and BMI [<i>β</i> coefficient = 3.747 (95% CI 1.013, 6.842); <i>p</i> < 0.01]. In SSc-patients without ILD, CWMA represents an important variable in exercise capacity and can be evaluated by the mediastinal window available in the HRCT images required for lung disease staging.</p>","PeriodicalId":13662,"journal":{"name":"Internal and Emergency Medicine","volume":"20 1","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2024-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Internal and Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11739-024-03751-z","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
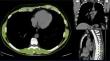
To investigate the potential contribution of chest wall muscle area (CWMA) to the ventilatory efficiency and exercise capacity in patients with Systemic Sclerosis (SSc) without interstitial lung disease (ILD). Forty-four consecutive SSc patients [F = 37, median age 53.5 years (IQR 43.5–58)] were examined using chest high-resolution computed tomography (HRCT), pulmonary function tests and cardiopulmonary exercise testing (CPET). The CWMA was evaluated at the level of the ninth thoracic vertebra on CT images by two independent evaluators blinded to the patient information. CPET parameters analyzed were maximum oxygen uptake (VO2 max) and VO2 at anaerobic threshold (VO2@AT); minute ventilation (VE); maximum tidal volume (VT). A statistically significant positive correlation was found between CWMA and maximum workload (r = 0.470, p < 0.01), VO2 max ml/min (r = 0.380, p < 0.01), VO2@AT (r = 0.343, p < 0.05), VE (r = 0.308, p < 0.05), VT (r = 0.410, p < 0.01) and VO2/heart rate (r = 0.399, p < 0.01). In multiple regression analysis, VO2 max (ml/min) was significantly associated with CWMA [β coefficient = 5.226 (95% CI 2.824, 7.628); p < 0.001], diffusing capacity for carbon monoxide (DLco) [β coefficient = 6.749 (95% CI 1.460, 12.039); p < 0.05] and body mass index (BMI) [β coefficient = 41.481 (95% CI 8.802, 74.161); p < 0.05]. In multiple regression analysis, maximum workload was significantly associated with CWMA [β coefficient = 0.490 (95% CI 0.289, 0.691); p < 0.001], DLco [β coefficient = 0.645 (95% CI 0.202, 1.088); p < 0.01] and BMI [β coefficient = 3.747 (95% CI 1.013, 6.842); p < 0.01]. In SSc-patients without ILD, CWMA represents an important variable in exercise capacity and can be evaluated by the mediastinal window available in the HRCT images required for lung disease staging.
期刊介绍:
Internal and Emergency Medicine (IEM) is an independent, international, English-language, peer-reviewed journal designed for internists and emergency physicians. IEM publishes a variety of manuscript types including Original investigations, Review articles, Letters to the Editor, Editorials and Commentaries. Occasionally IEM accepts unsolicited Reviews, Commentaries or Editorials. The journal is divided into three sections, i.e., Internal Medicine, Emergency Medicine and Clinical Evidence and Health Technology Assessment, with three separate editorial boards. In the Internal Medicine section, invited Case records and Physical examinations, devoted to underlining the role of a clinical approach in selected clinical cases, are also published. The Emergency Medicine section will include a Morbidity and Mortality Report and an Airway Forum concerning the management of difficult airway problems. As far as Critical Care is becoming an integral part of Emergency Medicine, a new sub-section will report the literature that concerns the interface not only for the care of the critical patient in the Emergency Department, but also in the Intensive Care Unit. Finally, in the Clinical Evidence and Health Technology Assessment section brief discussions of topics of evidence-based medicine (Cochrane’s corner) and Research updates are published. IEM encourages letters of rebuttal and criticism of published articles. Topics of interest include all subjects that relate to the science and practice of Internal and Emergency Medicine.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
