{"title":"Development of a system to support information sharing for medical staff in the hybrid emergency room","authors":"Shuhei Maruyama, Yasushi Nakamori, Shuji Kanayama, Daiki Wada, Fukuki Saito, Yasuyuki Kuwagata","doi":"10.1002/ams2.70006","DOIUrl":null,"url":null,"abstract":"<p>The hybrid ER<span><sup>1-3</sup></span> can significantly reduce time required for initial emergency care, but extensive information gathered during treatment needs to be interpreted and reflected in the treatment strategy within a short period of time. We report on the development of an information sharing system for initial emergency care.</p><p>During initial emergency care, vital signs, blood gas analysis (BGA), and laboratory data are important factors in decision making. When we perform surgery or transcatheter arterial embolization (TAE), knowing the trend of each parameter is important in determining whether vital signs have stabilized or worsened as a result of the therapeutic intervention. Vital sign monitors provide real-time vital signs but no information on their trend. In contrast, information systems commonly used in the intensive care unit or operating room provide trend information, but they update at a minimum of every minute. Updating at a minimum of every minute is too long for initial emergency care in which the critical patient's condition is constantly changing. Our developed system displays trend information on heart rate, blood pressure, and BGA that updates every 5 s and shows their trends over 180 min. Medical staff may not notice sudden changes in vital signs or results of BGA or laboratory data. When vital signs exceed a predetermined threshold, the system alerts them through an audio signal in the ER and in headsets and provides specific values for the medical staff. When updated results of BGA and laboratory tests are received, they are automatically and promptly showed in the monitor and read out as well. The manager could set any items in BGA and laboratory data to be read out by this system to their liking (e.g., calcium ions, CO-Hb). This allows the staff to recognize changes in vital signs and test results with no time lag. Initial emergency care, especially in trauma patients, is always a race against time. The system displays the time since the start of monitoring, surgery, TAE, and aortic blockade in a count-up format and alerts the medical staff via audio of the time that has elapsed. The system has two modes: standard mode and critical care specific (Figure 1 and Videos S1–S5). It responds to requests input through icons on the touch screen or by voice. This interactive utility is used to record various procedures, start and end times of measurements, and reconfirm information. Monitoring the administration of blood transfusion could be difficult in the emergency setting. The system displays administered transfusions (e.g., RBC, FFP, PC and cryoprecipitate) as the icons on the monitor manual input. In this way, the changes in vital signs and laboratory tests due to transfusion could be recognized on the screen. Dynamic monitoring updated every 5 s of vital signs are displayed on a 55-inch monitor so that staff can check the trend at any time and be alerted to changes in the patient's condition. We believe this system to be highly useful in improving functionality of the hybrid ER and enhancing the rate of life saving.</p><p>Shuhei Maruyama received lecture fees from Canon Medical Systems Co. Dr. Yasushi Nakamori received research grants from Canon Medical Systems Co. Dr. Yasuyuki Kuwagata is an Editorial Board member of the <i>Acute Medicine & Surgery</i> journal and a coauthor of this article. To minimize bias, he was excluded from all editorial decision-making related to the acceptance of this article for publication.</p><p>Approval of the research protocol: This study was conducted according to the principles of the Declaration of Helsinki and approved by Kansai Medical University Medical Center Institutional Review Board (Study Number: 2023283).</p><p>Informed consent: N/A.</p><p>Registry and the registration no. of the study/trial: N/A.</p><p>Animal studies: N/A.</p>","PeriodicalId":7196,"journal":{"name":"Acute Medicine & Surgery","volume":"11 1","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2024-09-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ams2.70006","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute Medicine & Surgery","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ams2.70006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
The hybrid ER1-3 can significantly reduce time required for initial emergency care, but extensive information gathered during treatment needs to be interpreted and reflected in the treatment strategy within a short period of time. We report on the development of an information sharing system for initial emergency care.
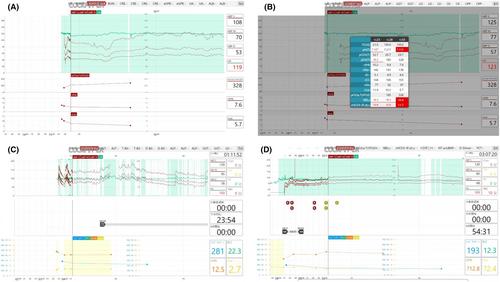
During initial emergency care, vital signs, blood gas analysis (BGA), and laboratory data are important factors in decision making. When we perform surgery or transcatheter arterial embolization (TAE), knowing the trend of each parameter is important in determining whether vital signs have stabilized or worsened as a result of the therapeutic intervention. Vital sign monitors provide real-time vital signs but no information on their trend. In contrast, information systems commonly used in the intensive care unit or operating room provide trend information, but they update at a minimum of every minute. Updating at a minimum of every minute is too long for initial emergency care in which the critical patient's condition is constantly changing. Our developed system displays trend information on heart rate, blood pressure, and BGA that updates every 5 s and shows their trends over 180 min. Medical staff may not notice sudden changes in vital signs or results of BGA or laboratory data. When vital signs exceed a predetermined threshold, the system alerts them through an audio signal in the ER and in headsets and provides specific values for the medical staff. When updated results of BGA and laboratory tests are received, they are automatically and promptly showed in the monitor and read out as well. The manager could set any items in BGA and laboratory data to be read out by this system to their liking (e.g., calcium ions, CO-Hb). This allows the staff to recognize changes in vital signs and test results with no time lag. Initial emergency care, especially in trauma patients, is always a race against time. The system displays the time since the start of monitoring, surgery, TAE, and aortic blockade in a count-up format and alerts the medical staff via audio of the time that has elapsed. The system has two modes: standard mode and critical care specific (Figure 1 and Videos S1–S5). It responds to requests input through icons on the touch screen or by voice. This interactive utility is used to record various procedures, start and end times of measurements, and reconfirm information. Monitoring the administration of blood transfusion could be difficult in the emergency setting. The system displays administered transfusions (e.g., RBC, FFP, PC and cryoprecipitate) as the icons on the monitor manual input. In this way, the changes in vital signs and laboratory tests due to transfusion could be recognized on the screen. Dynamic monitoring updated every 5 s of vital signs are displayed on a 55-inch monitor so that staff can check the trend at any time and be alerted to changes in the patient's condition. We believe this system to be highly useful in improving functionality of the hybrid ER and enhancing the rate of life saving.
Shuhei Maruyama received lecture fees from Canon Medical Systems Co. Dr. Yasushi Nakamori received research grants from Canon Medical Systems Co. Dr. Yasuyuki Kuwagata is an Editorial Board member of the Acute Medicine & Surgery journal and a coauthor of this article. To minimize bias, he was excluded from all editorial decision-making related to the acceptance of this article for publication.
Approval of the research protocol: This study was conducted according to the principles of the Declaration of Helsinki and approved by Kansai Medical University Medical Center Institutional Review Board (Study Number: 2023283).
Informed consent: N/A.
Registry and the registration no. of the study/trial: N/A.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
