Prognostic role of dynamic changes in inflammatory indicators in patients with non-small cell lung cancer treated with immune checkpoint inhibitors-a retrospective cohort study.
{"title":"Prognostic role of dynamic changes in inflammatory indicators in patients with non-small cell lung cancer treated with immune checkpoint inhibitors-a retrospective cohort study.","authors":"Liang Guo, Juanjuan Li, Jing Wang, Xinru Chen, Chenlei Cai, Fei Zhou, Anwen Xiong","doi":"10.21037/tlcr-24-637","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Immune checkpoint inhibitors (ICIs) have become one of the standard treatments for non-small cell lung cancer (NSCLC) patients without driver mutations. However, a considerable proportion of patients suffer from severe immune side effects and fail to respond to ICIs. As effective biomarkers, programmed cell death ligand 1 (PD-L1) expression, microsatellite instability (MSI), the tumor mutation burden (TMB) and tumor-infiltrating lymphocytes (TILs) require invasive procedures that place heavy physical and psychological burdens on patients. This study aims to identify simple and effective markers to optimize patient selection through therapeutic decisions and outcome prediction.</p><p><strong>Methods: </strong>This retrospective study comprised 95 patients with metastatic NSCLC who were treated with ICIs either as the standard of care or in a clinical trial. The following data were extracted from the medical records. The baseline and dynamic neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) were calculated in the present study. Responses were assessed by computed tomography (CT) imaging and classified according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 every 6-12 weeks during treatment.</p><p><strong>Results: </strong>In total, 95 patients were included in the present study. The median age of patients was 61 years, 83.2% (79/95) patients were male, 62.1% (59/95) were former or current smokers, 66.3% (63/95) had adenocarcinoma, 93.7% (89/95) had stage IV disease, and 87.4% were without molecular alterations. A higher overall response rate (ORR) and prolonged median progression-free survival (PFS) was observed in patients with a lower cycle 3 (C3) NLR [7.7 <i>vs.</i> 5.5 months, hazard ratio (HR): 1.70, 95% confidence interval (CI): 0.90-3.22; P=0.12] and derived NLR (dNLR) (8.2 <i>vs.</i> 5.6 months, HR: 1.67, 95% CI: 0.94-2.97; P=0.08). After two cycles of ICI treatment, patients who had an increased NLR, dNLR, and PLR had a lower ORR and an inferior median PFS than those with a decreased NLR (5.5 <i>vs.</i> 8.5 months, HR: 1.87, 95% CI: 1.09-3.21; P=0.02), dNLR (5.6 <i>vs.</i> 8.4 months, HR: 1.49, 95% CI: 0.87-2.57; P=0.15), and PLR (11.8 <i>vs.</i> 5.5 months, HR: 2.28, 95% CI: 1.32-3.94; P=0.003). Moreover, patients with both an increased NLR and PLR had a worse ORR and median PFS than those with either an increased NLR or PLR, or both an increased NLR and PLR (11.8 <i>vs.</i> 5.5 <i>vs.</i> 5.6 months, P=0.003). In addition, the dynamic changes in the PLR could serve as an independent predictive factor of PFS in NSCLC patients treated with ICIs.</p><p><strong>Conclusions: </strong>Elevated dynamic changes in the NLR and PLR were associated with lower response rates and shorter PFS in the patients with NSCLC treated with ICIs. Our results also highlight the role of dynamic changes in the PLR in identifying patients with NSCLC who could benefit from ICIs.</p>","PeriodicalId":23271,"journal":{"name":"Translational lung cancer research","volume":"13 8","pages":"1975-1987"},"PeriodicalIF":3.5000,"publicationDate":"2024-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11384502/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational lung cancer research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tlcr-24-637","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/28 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Immune checkpoint inhibitors (ICIs) have become one of the standard treatments for non-small cell lung cancer (NSCLC) patients without driver mutations. However, a considerable proportion of patients suffer from severe immune side effects and fail to respond to ICIs. As effective biomarkers, programmed cell death ligand 1 (PD-L1) expression, microsatellite instability (MSI), the tumor mutation burden (TMB) and tumor-infiltrating lymphocytes (TILs) require invasive procedures that place heavy physical and psychological burdens on patients. This study aims to identify simple and effective markers to optimize patient selection through therapeutic decisions and outcome prediction.
Methods: This retrospective study comprised 95 patients with metastatic NSCLC who were treated with ICIs either as the standard of care or in a clinical trial. The following data were extracted from the medical records. The baseline and dynamic neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) were calculated in the present study. Responses were assessed by computed tomography (CT) imaging and classified according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 every 6-12 weeks during treatment.
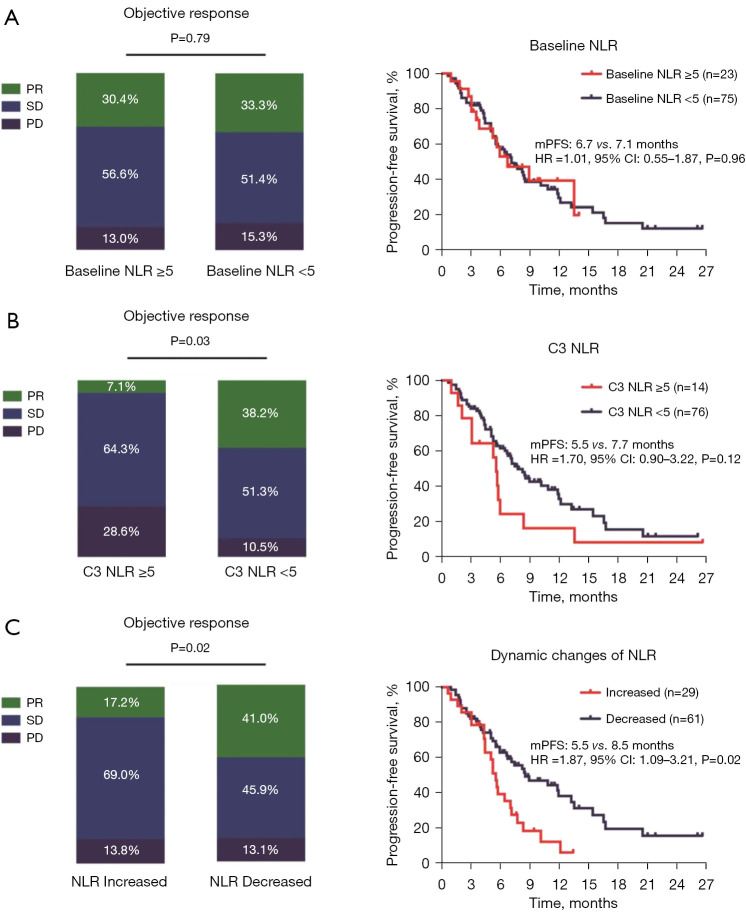
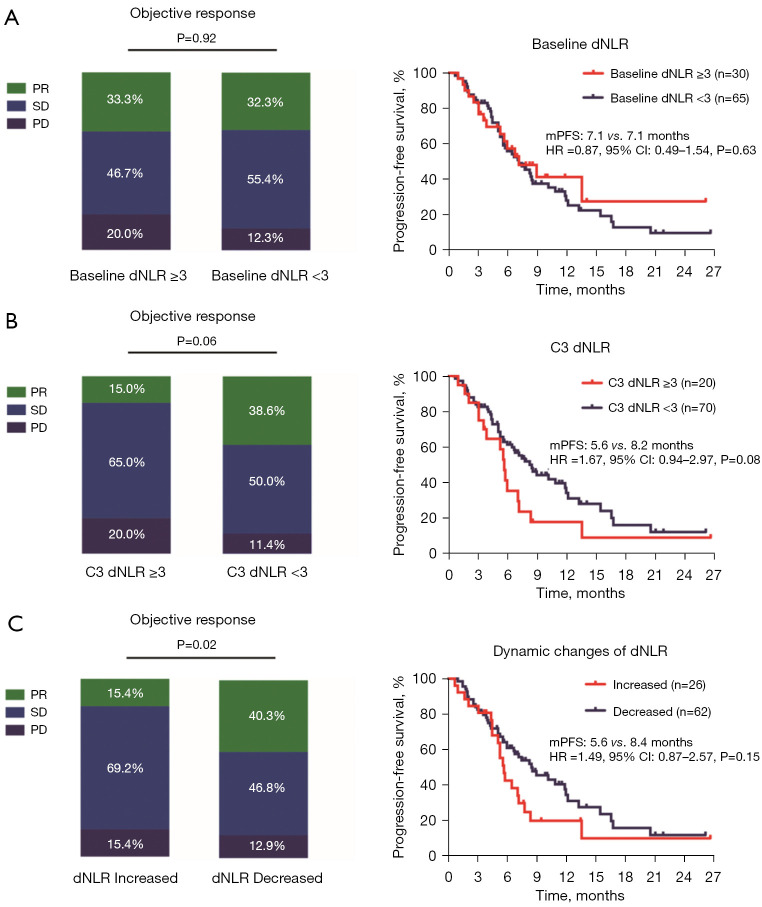
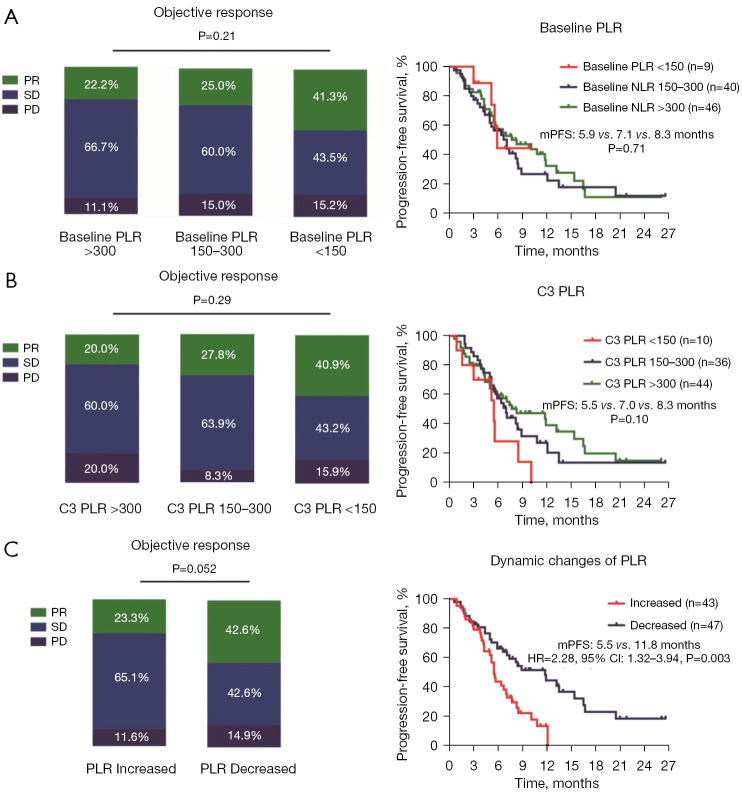
Results: In total, 95 patients were included in the present study. The median age of patients was 61 years, 83.2% (79/95) patients were male, 62.1% (59/95) were former or current smokers, 66.3% (63/95) had adenocarcinoma, 93.7% (89/95) had stage IV disease, and 87.4% were without molecular alterations. A higher overall response rate (ORR) and prolonged median progression-free survival (PFS) was observed in patients with a lower cycle 3 (C3) NLR [7.7 vs. 5.5 months, hazard ratio (HR): 1.70, 95% confidence interval (CI): 0.90-3.22; P=0.12] and derived NLR (dNLR) (8.2 vs. 5.6 months, HR: 1.67, 95% CI: 0.94-2.97; P=0.08). After two cycles of ICI treatment, patients who had an increased NLR, dNLR, and PLR had a lower ORR and an inferior median PFS than those with a decreased NLR (5.5 vs. 8.5 months, HR: 1.87, 95% CI: 1.09-3.21; P=0.02), dNLR (5.6 vs. 8.4 months, HR: 1.49, 95% CI: 0.87-2.57; P=0.15), and PLR (11.8 vs. 5.5 months, HR: 2.28, 95% CI: 1.32-3.94; P=0.003). Moreover, patients with both an increased NLR and PLR had a worse ORR and median PFS than those with either an increased NLR or PLR, or both an increased NLR and PLR (11.8 vs. 5.5 vs. 5.6 months, P=0.003). In addition, the dynamic changes in the PLR could serve as an independent predictive factor of PFS in NSCLC patients treated with ICIs.
Conclusions: Elevated dynamic changes in the NLR and PLR were associated with lower response rates and shorter PFS in the patients with NSCLC treated with ICIs. Our results also highlight the role of dynamic changes in the PLR in identifying patients with NSCLC who could benefit from ICIs.
期刊介绍:
Translational Lung Cancer Research(TLCR, Transl Lung Cancer Res, Print ISSN 2218-6751; Online ISSN 2226-4477) is an international, peer-reviewed, open-access journal, which was founded in March 2012. TLCR is indexed by PubMed/PubMed Central and the Chemical Abstracts Service (CAS) Databases. It is published quarterly the first year, and published bimonthly since February 2013. It provides practical up-to-date information on prevention, early detection, diagnosis, and treatment of lung cancer. Specific areas of its interest include, but not limited to, multimodality therapy, markers, imaging, tumor biology, pathology, chemoprevention, and technical advances related to lung cancer.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
