Nikoleta Bizymi, Athina Damianaki, Nikoletta Aresti, Anastasios Karasachinidis, Zacharenia Vlata, Matthieu Lavigne, Emmanuel Dialynas, Niki Gounalaki, Irene Stratidaki, Grigorios Tsaknakis, Aristea Batsali, Irene Mavroudi, Maria Velegraki, Ioannis Sperelakis, Charalampos Pontikoglou, Panayotis Verginis, Helen A. Papadaki
{"title":"Characterization of myeloid-derived suppressor cells in the peripheral blood and bone marrow of patients with chronic idiopathic neutropenia","authors":"Nikoleta Bizymi, Athina Damianaki, Nikoletta Aresti, Anastasios Karasachinidis, Zacharenia Vlata, Matthieu Lavigne, Emmanuel Dialynas, Niki Gounalaki, Irene Stratidaki, Grigorios Tsaknakis, Aristea Batsali, Irene Mavroudi, Maria Velegraki, Ioannis Sperelakis, Charalampos Pontikoglou, Panayotis Verginis, Helen A. Papadaki","doi":"10.1002/hem3.70005","DOIUrl":null,"url":null,"abstract":"<p>Chronic idiopathic neutropenia (CIN) is characterized by the persistent and unexplained reduction of peripheral blood (PB) absolute neutrophil counts (ANCs).<span><sup>1, 2</sup></span> The pathogenesis of CIN has been associated with increased apoptosis of the granulocytic progenitor cells due to an inflammatory bone marrow (BM) microenvironment consisting of activated T lymphocytes, proinflammatory monocytes, and proapoptotic cytokines.<span><sup>3-5</sup></span> The myeloid-derived suppressor cells (MDSCs) are immature myeloid cells, deviating from the standard differentiation pathway during emergency myelopoiesis, that display immunomodulatory properties mainly by suppressing T-cell responses. They are recognized by the immunophenotype CD11b<sup>+</sup>CD33<sup>+</sup>HLA-DR<sup>–/low</sup> and further characterized as CD14<sup>+</sup> (monocytic, M-MDSCs) and CD15<sup>+</sup> (polymorphonuclear, PMN-MDSCs) subpopulations.<span><sup>6-13</sup></span></p><p>In the present study, we explore, for the first time, the possible involvement of MDSCs in the pathophysiology of CIN by investigating their number, functional characteristics, and transcriptome profile in a group of patients (<i>n</i> = 102) and age- and sex-matched healthy controls (<i>n</i> = 77). The patients fulfilled the previously described diagnostic criteria for CIN (File S1).<span><sup>2, 14, 15</sup></span> Sixteen patients had clonal hematopoiesis identified by next-generation sequencing analysis of 40 recurrently mutated myeloid genes.<span><sup>15</sup></span> The clinical and laboratory data of the patients are presented in Supporting Information S1: Tables 1 and 2. The study was approved by the Institutional Review Board of the University Hospital of Heraklion and informed consent was obtained from all subjects.</p><p>MDSC subsets were quantitated and sorted by flow cytometry in the PB mononuclear cell (PBMC) and BM mononuclear cell (BMMC) fractions according to the recommended protocol.<span><sup>6</sup></span> The gating strategies for MDSC quantification and sorting are presented in Figure 1A,B respectively. The methodology of the T-cell suppression assay to evaluate the function of MDSCs was performed according to the recommended standards (File S1).<span><sup>6, 18, 19</sup></span> In brief, the suppression of normal T cells was demonstrated in a heterologous system including co-culture of immunomagnetically sorted carboxy-fluorescein succinimidyl ester (CFSE)-stained T cells with PMN-MDSCs or M-MDSCs (Figure 1C) and an autologous system including cultures of CFSE-stained PBMCs versus CD33-immunomagnetically depleted PBMCs (Figure 1D). To identify the biochemical and molecular parameters associated with MDSC characterization,<span><sup>6</sup></span> we performed transcriptional profiling of MDSCs from patients (<i>n</i> = 6) and healthy controls (<i>n</i> = 5) using RNA sequencing (File S1 and Supporting Information S1: Table 3). The data were analyzed using the GraphPad Prism Statistical software with the nonparametric Mann–Whitney <i>U</i> test, the Wilcoxon signed ranks test for paired samples, and the Kruskal–Wallis test for comparison between multiple groups. The Spearman test was used for the identification of correlations between different parameters. Data are presented as mean value ± 1 standard deviation.</p><p>We found that CIN patients displayed significantly lower proportions of MDSCs in both the PBMC (<i>n</i> = 102) and BMMC (<i>n</i> = 37) fractions compared to healthy controls (<i>n</i> = 77 and <i>n</i> = 8, respectively) (Table 1). The proportion of PB total MDSCs (T-MDSCs: PMN-MDSCs plus M-MDSCs) was statistically significantly lower in patients compared to controls (<i>p</i> < 0.0001). This decrease was due to the lower proportion of both PMN-MDSC and M-MDSC subsets in patients compared to controls (<i>p</i> = 0.0298 and <i>p</i> < 0.0001, respectively) (Table 1 and Figure 1E,F). The proportions of T-MDSCs and their subsets, that is, the PMN-MDSCs and M-MDSCs, were correlated with the ANCs in the total group of subjects studied (<i>r</i> = 0.399, <i>p</i> < 0.0001; <i>r</i> = 0.1757, <i>p</i> = 0.0219; <i>r</i> = 0.4115, <i>p</i> < 0.0001, respectively) (Supporting Information S1: Figures 1A–C). However, when a subset analysis was performed in the group of patients only, no correlation was identified between MDSC subsets and ANCs, suggesting that apparently more factors are involved in the development of neutropenia in CIN. In favor of this assumption, the proportions of T-MDSCs, PMN-MDSCs, and M-MDSCs were not statistically significantly different between patients with mild (ANC ≥ 1.0 × 10<sup>9</sup>/L) and more severe (ANC < 1.0 × 10<sup>9</sup>/L) neutropenia (Table 1). Both patient groups, that is, patients with mild (<i>n</i> = 77) and more severe (<i>n</i> = 25) neutropenia, displayed significantly lower T-MDSC proportions compared to healthy individuals (<i>p</i> < 0.0001 and <i>p</i> = 0.0002, respectively), mainly due to the lower proportions of M-MDSCs (<i>p</i> < 0.0001 and <i>p</i> = 0.0002, respectively). PMN-MDSC proportions were also lower in both patient groups compared to healthy individuals, but the decrease was more profound in the group with mild neutropenia (<i>p</i> = 0.045), apparently due to the higher number of patients in this group (Table 1). As expected, given that M-MDSCs are part of the monocytes, the proportions of M-MDSCs were correlated with the absolute monocyte counts in both the total study population (<i>r</i> = 0.4197, <i>p</i> < 0.0001) and the CIN group (<i>r</i> = 0.3566, <i>p</i> = 0.0002). Finally, a subset analysis was performed in MDSC subsets between patients with clonal and non-clonal hematopoiesis (Supporting Information S1: Table 4). No statistically significant difference was identified between these patient groups, suggesting that the MDSC numbers are not associated with the presence of clonal disease in CIN. The proportion of T-MDSCs in the BMMC fraction was significantly lower in patients compared to controls (<i>p</i> = 0.0312) (Table 1). The subset analysis showed that both PMN-MDSC and M-MDSC proportions were significantly lower in the patients compared to controls (<i>p</i> = 0.0312 and <i>p</i> = 0.0369, respectively) (Table 1 and Figure 1G,H). These data indicate defective ΒΜ production of PMN-MDSCs and M-MDSCs in CIN patients compared to healthy individuals.</p><p>CIN patient MDSCs displayed normal T-cell suppressive activity. In the total set of experiments evaluating the T-cell suppressive activity of patient MDSCs, the undivided cells in the cultures were significantly increased in the presence of MDSCs (1.58% ± 4.61%, median 0.02%, range 0%−20.31%) compared to those with absence of MDSCs (0.34% ± 1.51%, median 0.00%, range 0%−7.09%) (<i>p</i> = 0.001) (Supporting Information S1: Figure 2A). There were no statistically significant differences in the proportion of undivided cells between PMN-MDSCs (0.14% ± 0.20%, median 0.02%, range 0%−0.47%) and M-MDSCs (0.48% ± 0.75%, median 0.03%, range 0%−1.74%, <i>p</i> = 0.5) or between healthy (0.39% ± 0.69%, median 0.00%, range 0%−1.96%) and CIN cultures (1.83% ± 5.48%, median 0.06%, range 0%−19.99%, <i>p</i> = 0.4821) (Supporting Information S1: Figure 2B,C).</p><p>Τhe transcriptomic analysis of MDSCs from CIN patients showed an altered profile compared to healthy individuals. A significant number of mapped reads (1202 for PMN-MDSCs and 239 for M-MDSCs) were differentially expressed (log2fold change (FC) ≥ | 2| and <i>p</i> < 0.05) between patients and controls. In patient PMN-MDSCs and M-MDSCs, 524 and 162 mapped reads, respectively, were upregulated, whereas 678 and 77 mapped reads, respectively, were downregulated. All differentially expressed mapped reads are given in Supporting Information S1: Tables 5 and 6. Patient and control MDSCs expressed genes typically associated with their immunomodulatory properties. Specifically, the genes of S100 calcium-binding protein A8/A9 (S100A8/A9) and nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB), which are typically associated with MDSC immunomodulatory properties, were among the most highly expressed sequences in both patients and controls (Figure 1I). However, alternative genes associated with MDSC expansion, phenotype, and functionality were downregulated (<i>CEBPB</i>, <i>TGFBR2</i>, <i>VEGFB</i>, <i>IL4R</i>), while others, such as <i>IRF8</i>, which is typically expressed at a low level in normal MDSCs, were upregulated in patient MDSCs. Taken together, the transcriptomic analysis<span><sup>17</sup></span> revealed that MDSCs from CIN patients, compared to those from healthy controls, display an altered immunomodulatory profile associated with upregulation of pathways related to inflammatory responses (e.g., <i>IL6</i>, <i>IL1B</i>, <i>CCR2</i>, <i>CD86</i>) and T-cell activation/responses (e.g., <i>IL6</i>, <i>CD28</i>) and downregulation of genes related to cellular viability and responses to damage (e.g., <i>POLB, RPA4, ERCC4</i>) and phagocytic functions (e.g., <i>BLTP1</i>, <i>ABCA1</i>, <i>NCF4</i>) (Figure 1J,K and Supporting Information S1: Figure 3).</p><p>Overall, we have shown that CIN patients have significantly lower proportions of MDSCs in the PBMC and BMMC fractions compared to healthy controls. MDSCs of CIN patients sufficiently suppress T cells <i>ex vivo</i> but display altered transcriptome properties implying intrinsic functional defects, beyond the T-cell suppression capacity, <i>in vivo</i>. Interestingly, low numbers of MDSCs and abnormal transcriptome profiles associated with intrinsic defects of MDSCs such as downregulation of genes related to responses to inflammatory cytokines and upregulation of genes related to DNA damage and apoptosis have been also found in patients with aplastic anemia and these defects have been associated with the immunopathogenesis of the disease.<span><sup>20</sup></span> The downregulation of genes related to MDSC expansion (e.g., <i>CEBPB</i>), along with the contracted BM myeloid progenitor cell compartment,<span><sup>3</sup></span> may have a role in the defective MDSC production in CIN patients. A higher apoptotic rate of MDSCs might be an additional mechanism for the decreased MDSC numbers in CIN as was indicated by the higher transcriptome expression of genes related to apoptosis (e.g., <i>DAPK2</i>) and lower expression of genes related to cell viability and repair after stress (e.g., <i>POLB, RPA4, ERCC4</i>), compared to healthy individuals. The low numbers and altered properties of MDSCs probably result in inadequate suppression of the aberrant inflammatory processes known to underlie CIN, contributing therefore to the increased levels of circulating inflammatory cytokines and chemokines. Our results depict for the first time the alterations of MDSCs in CIN and trigger more mechanistic studies in the future to further explore the exact role of these cells in the disease.</p><p>Nikoleta Bizymi performed the laboratory work, analyzed the data, wrote the paper, and participated in research design. Athina Damianaki, Anastasios Karasachinidis, Nikoletta Aresti, Grigorios Tsaknakis, Aristea Batsali, and Irene Mavroudi performed laboratory work. Maria Velegraki participated in the research design and in the performance of research. Zacharenia Vlata, Ioannis Sperelakis, Matthieu Lavigne, Emmanuel Dialynas, Niki Gounalaki, and Irene Stratidaki performed research and data analysis. Charalampos Pontikoglou and Panayotis Verginis participated in the research design. Helen A. Papadaki designed and supervised the study, provided the patient samples, analyzed and interpreted the data, and wrote the paper. All authors have read and agreed to the final version of the manuscript.</p><p>The authors declare no conflict of interest.</p><p>This work was supported by the Alexander S. Onassis Public Benefit Foundation in Greece Scholarship G NZ 035-1/2017-2018 to N. B. for master studies and the Maria Michail Manassaki Scholarship of the University of Crete to N. B. for PhD studies. It was also based upon work from the COST Actions BM1404—European Network of Investigators Triggering Exploratory Research on Myeloid Regulatory Cells (Mye-EUNITER) and CA18233—European Network for Innovative Diagnosis and Treatment of Chronic Neutropenias (EuNet-INNOCHRON) supported by COST (European Cooperation in Science and Technology).</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 9","pages":""},"PeriodicalIF":7.6000,"publicationDate":"2024-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11417472/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.70005","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Chronic idiopathic neutropenia (CIN) is characterized by the persistent and unexplained reduction of peripheral blood (PB) absolute neutrophil counts (ANCs).1, 2 The pathogenesis of CIN has been associated with increased apoptosis of the granulocytic progenitor cells due to an inflammatory bone marrow (BM) microenvironment consisting of activated T lymphocytes, proinflammatory monocytes, and proapoptotic cytokines.3-5 The myeloid-derived suppressor cells (MDSCs) are immature myeloid cells, deviating from the standard differentiation pathway during emergency myelopoiesis, that display immunomodulatory properties mainly by suppressing T-cell responses. They are recognized by the immunophenotype CD11b+CD33+HLA-DR–/low and further characterized as CD14+ (monocytic, M-MDSCs) and CD15+ (polymorphonuclear, PMN-MDSCs) subpopulations.6-13
In the present study, we explore, for the first time, the possible involvement of MDSCs in the pathophysiology of CIN by investigating their number, functional characteristics, and transcriptome profile in a group of patients (n = 102) and age- and sex-matched healthy controls (n = 77). The patients fulfilled the previously described diagnostic criteria for CIN (File S1).2, 14, 15 Sixteen patients had clonal hematopoiesis identified by next-generation sequencing analysis of 40 recurrently mutated myeloid genes.15 The clinical and laboratory data of the patients are presented in Supporting Information S1: Tables 1 and 2. The study was approved by the Institutional Review Board of the University Hospital of Heraklion and informed consent was obtained from all subjects.
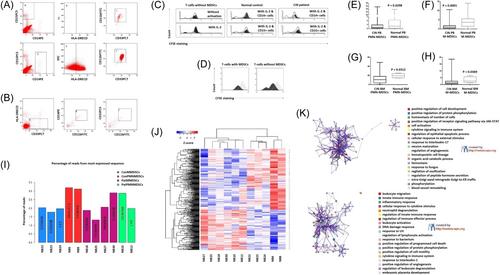
MDSC subsets were quantitated and sorted by flow cytometry in the PB mononuclear cell (PBMC) and BM mononuclear cell (BMMC) fractions according to the recommended protocol.6 The gating strategies for MDSC quantification and sorting are presented in Figure 1A,B respectively. The methodology of the T-cell suppression assay to evaluate the function of MDSCs was performed according to the recommended standards (File S1).6, 18, 19 In brief, the suppression of normal T cells was demonstrated in a heterologous system including co-culture of immunomagnetically sorted carboxy-fluorescein succinimidyl ester (CFSE)-stained T cells with PMN-MDSCs or M-MDSCs (Figure 1C) and an autologous system including cultures of CFSE-stained PBMCs versus CD33-immunomagnetically depleted PBMCs (Figure 1D). To identify the biochemical and molecular parameters associated with MDSC characterization,6 we performed transcriptional profiling of MDSCs from patients (n = 6) and healthy controls (n = 5) using RNA sequencing (File S1 and Supporting Information S1: Table 3). The data were analyzed using the GraphPad Prism Statistical software with the nonparametric Mann–Whitney U test, the Wilcoxon signed ranks test for paired samples, and the Kruskal–Wallis test for comparison between multiple groups. The Spearman test was used for the identification of correlations between different parameters. Data are presented as mean value ± 1 standard deviation.
We found that CIN patients displayed significantly lower proportions of MDSCs in both the PBMC (n = 102) and BMMC (n = 37) fractions compared to healthy controls (n = 77 and n = 8, respectively) (Table 1). The proportion of PB total MDSCs (T-MDSCs: PMN-MDSCs plus M-MDSCs) was statistically significantly lower in patients compared to controls (p < 0.0001). This decrease was due to the lower proportion of both PMN-MDSC and M-MDSC subsets in patients compared to controls (p = 0.0298 and p < 0.0001, respectively) (Table 1 and Figure 1E,F). The proportions of T-MDSCs and their subsets, that is, the PMN-MDSCs and M-MDSCs, were correlated with the ANCs in the total group of subjects studied (r = 0.399, p < 0.0001; r = 0.1757, p = 0.0219; r = 0.4115, p < 0.0001, respectively) (Supporting Information S1: Figures 1A–C). However, when a subset analysis was performed in the group of patients only, no correlation was identified between MDSC subsets and ANCs, suggesting that apparently more factors are involved in the development of neutropenia in CIN. In favor of this assumption, the proportions of T-MDSCs, PMN-MDSCs, and M-MDSCs were not statistically significantly different between patients with mild (ANC ≥ 1.0 × 109/L) and more severe (ANC < 1.0 × 109/L) neutropenia (Table 1). Both patient groups, that is, patients with mild (n = 77) and more severe (n = 25) neutropenia, displayed significantly lower T-MDSC proportions compared to healthy individuals (p < 0.0001 and p = 0.0002, respectively), mainly due to the lower proportions of M-MDSCs (p < 0.0001 and p = 0.0002, respectively). PMN-MDSC proportions were also lower in both patient groups compared to healthy individuals, but the decrease was more profound in the group with mild neutropenia (p = 0.045), apparently due to the higher number of patients in this group (Table 1). As expected, given that M-MDSCs are part of the monocytes, the proportions of M-MDSCs were correlated with the absolute monocyte counts in both the total study population (r = 0.4197, p < 0.0001) and the CIN group (r = 0.3566, p = 0.0002). Finally, a subset analysis was performed in MDSC subsets between patients with clonal and non-clonal hematopoiesis (Supporting Information S1: Table 4). No statistically significant difference was identified between these patient groups, suggesting that the MDSC numbers are not associated with the presence of clonal disease in CIN. The proportion of T-MDSCs in the BMMC fraction was significantly lower in patients compared to controls (p = 0.0312) (Table 1). The subset analysis showed that both PMN-MDSC and M-MDSC proportions were significantly lower in the patients compared to controls (p = 0.0312 and p = 0.0369, respectively) (Table 1 and Figure 1G,H). These data indicate defective ΒΜ production of PMN-MDSCs and M-MDSCs in CIN patients compared to healthy individuals.
CIN patient MDSCs displayed normal T-cell suppressive activity. In the total set of experiments evaluating the T-cell suppressive activity of patient MDSCs, the undivided cells in the cultures were significantly increased in the presence of MDSCs (1.58% ± 4.61%, median 0.02%, range 0%−20.31%) compared to those with absence of MDSCs (0.34% ± 1.51%, median 0.00%, range 0%−7.09%) (p = 0.001) (Supporting Information S1: Figure 2A). There were no statistically significant differences in the proportion of undivided cells between PMN-MDSCs (0.14% ± 0.20%, median 0.02%, range 0%−0.47%) and M-MDSCs (0.48% ± 0.75%, median 0.03%, range 0%−1.74%, p = 0.5) or between healthy (0.39% ± 0.69%, median 0.00%, range 0%−1.96%) and CIN cultures (1.83% ± 5.48%, median 0.06%, range 0%−19.99%, p = 0.4821) (Supporting Information S1: Figure 2B,C).
Τhe transcriptomic analysis of MDSCs from CIN patients showed an altered profile compared to healthy individuals. A significant number of mapped reads (1202 for PMN-MDSCs and 239 for M-MDSCs) were differentially expressed (log2fold change (FC) ≥ | 2| and p < 0.05) between patients and controls. In patient PMN-MDSCs and M-MDSCs, 524 and 162 mapped reads, respectively, were upregulated, whereas 678 and 77 mapped reads, respectively, were downregulated. All differentially expressed mapped reads are given in Supporting Information S1: Tables 5 and 6. Patient and control MDSCs expressed genes typically associated with their immunomodulatory properties. Specifically, the genes of S100 calcium-binding protein A8/A9 (S100A8/A9) and nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB), which are typically associated with MDSC immunomodulatory properties, were among the most highly expressed sequences in both patients and controls (Figure 1I). However, alternative genes associated with MDSC expansion, phenotype, and functionality were downregulated (CEBPB, TGFBR2, VEGFB, IL4R), while others, such as IRF8, which is typically expressed at a low level in normal MDSCs, were upregulated in patient MDSCs. Taken together, the transcriptomic analysis17 revealed that MDSCs from CIN patients, compared to those from healthy controls, display an altered immunomodulatory profile associated with upregulation of pathways related to inflammatory responses (e.g., IL6, IL1B, CCR2, CD86) and T-cell activation/responses (e.g., IL6, CD28) and downregulation of genes related to cellular viability and responses to damage (e.g., POLB, RPA4, ERCC4) and phagocytic functions (e.g., BLTP1, ABCA1, NCF4) (Figure 1J,K and Supporting Information S1: Figure 3).
Overall, we have shown that CIN patients have significantly lower proportions of MDSCs in the PBMC and BMMC fractions compared to healthy controls. MDSCs of CIN patients sufficiently suppress T cells ex vivo but display altered transcriptome properties implying intrinsic functional defects, beyond the T-cell suppression capacity, in vivo. Interestingly, low numbers of MDSCs and abnormal transcriptome profiles associated with intrinsic defects of MDSCs such as downregulation of genes related to responses to inflammatory cytokines and upregulation of genes related to DNA damage and apoptosis have been also found in patients with aplastic anemia and these defects have been associated with the immunopathogenesis of the disease.20 The downregulation of genes related to MDSC expansion (e.g., CEBPB), along with the contracted BM myeloid progenitor cell compartment,3 may have a role in the defective MDSC production in CIN patients. A higher apoptotic rate of MDSCs might be an additional mechanism for the decreased MDSC numbers in CIN as was indicated by the higher transcriptome expression of genes related to apoptosis (e.g., DAPK2) and lower expression of genes related to cell viability and repair after stress (e.g., POLB, RPA4, ERCC4), compared to healthy individuals. The low numbers and altered properties of MDSCs probably result in inadequate suppression of the aberrant inflammatory processes known to underlie CIN, contributing therefore to the increased levels of circulating inflammatory cytokines and chemokines. Our results depict for the first time the alterations of MDSCs in CIN and trigger more mechanistic studies in the future to further explore the exact role of these cells in the disease.
Nikoleta Bizymi performed the laboratory work, analyzed the data, wrote the paper, and participated in research design. Athina Damianaki, Anastasios Karasachinidis, Nikoletta Aresti, Grigorios Tsaknakis, Aristea Batsali, and Irene Mavroudi performed laboratory work. Maria Velegraki participated in the research design and in the performance of research. Zacharenia Vlata, Ioannis Sperelakis, Matthieu Lavigne, Emmanuel Dialynas, Niki Gounalaki, and Irene Stratidaki performed research and data analysis. Charalampos Pontikoglou and Panayotis Verginis participated in the research design. Helen A. Papadaki designed and supervised the study, provided the patient samples, analyzed and interpreted the data, and wrote the paper. All authors have read and agreed to the final version of the manuscript.
The authors declare no conflict of interest.
This work was supported by the Alexander S. Onassis Public Benefit Foundation in Greece Scholarship G NZ 035-1/2017-2018 to N. B. for master studies and the Maria Michail Manassaki Scholarship of the University of Crete to N. B. for PhD studies. It was also based upon work from the COST Actions BM1404—European Network of Investigators Triggering Exploratory Research on Myeloid Regulatory Cells (Mye-EUNITER) and CA18233—European Network for Innovative Diagnosis and Treatment of Chronic Neutropenias (EuNet-INNOCHRON) supported by COST (European Cooperation in Science and Technology).
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
