{"title":"L-Dopa Might Be Insufficient to Suppress Development of Prolactinomas in Dihydropteridine Reductase-Deficiency Patients.","authors":"Unai Diaz-Moreno, Cheng Guang Gan, Divya Pujari, Hoong-Wei Gan, Spyros Batzios","doi":"10.1210/jcemcr/luae172","DOIUrl":null,"url":null,"abstract":"<p><p>Dihydropteridine reductase (DHPR) deficiency is a disorder that prevents regeneration of tetrahydrobiopterin (BH4), causing hyperphenylalaninemia (HPA) and low levels of neurotransmitters, including dopamine. Due to low levels of dopamine, patients present with hyperprolactinemia. Treatment consists of a phenylalanine (Phe)-restricted diet, hydroxytryptophan and levodopa (L-Dopa) supplementation, leading to a rapid normalization of prolactin (PRL) levels. We report a case of a patient with DHPR deficiency presenting with new symptomatic hyperprolactinemia and amenorrhea in adolescence despite appropriate management. The prolactinoma was confirmed with pituitary magnetic resonance imaging. The patient was started on cabergoline with rapid normalization of PRL levels and resolution of symptoms, in keeping with previous reports. Cabergoline has a stronger affinity for the D2R receptor and longer half-life than L-Dopa, leading to lactotroph apoptosis, tumor shrinkage, and rapid and maintained normalization of PRL levels, with a better side-effect profile. Patients with DHPR deficiency need to be actively monitored for symptomatic hyperprolactinemia, as L-Dopa monotherapy is insufficient to suppress PRL secretion, leading to lactotroph hypertrophy and proliferation over time and development of prolactinomas in later life.</p>","PeriodicalId":73540,"journal":{"name":"JCEM case reports","volume":"2 10","pages":"luae172"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11427838/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCEM case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jcemcr/luae172","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
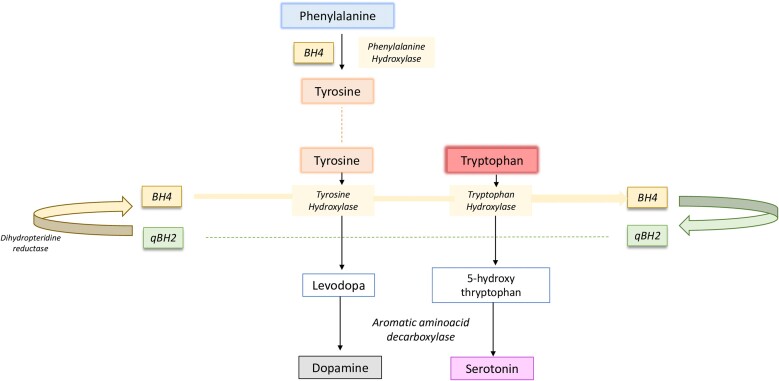
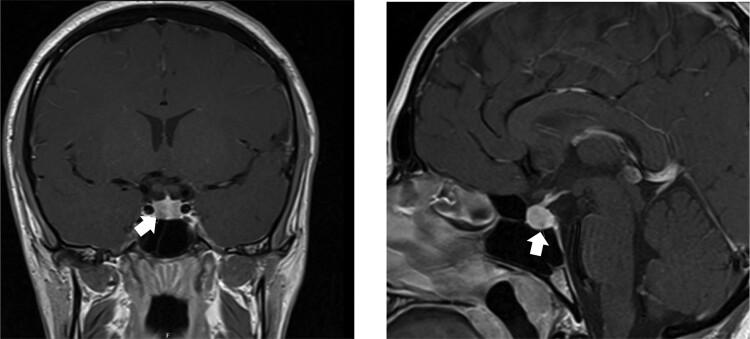
Dihydropteridine reductase (DHPR) deficiency is a disorder that prevents regeneration of tetrahydrobiopterin (BH4), causing hyperphenylalaninemia (HPA) and low levels of neurotransmitters, including dopamine. Due to low levels of dopamine, patients present with hyperprolactinemia. Treatment consists of a phenylalanine (Phe)-restricted diet, hydroxytryptophan and levodopa (L-Dopa) supplementation, leading to a rapid normalization of prolactin (PRL) levels. We report a case of a patient with DHPR deficiency presenting with new symptomatic hyperprolactinemia and amenorrhea in adolescence despite appropriate management. The prolactinoma was confirmed with pituitary magnetic resonance imaging. The patient was started on cabergoline with rapid normalization of PRL levels and resolution of symptoms, in keeping with previous reports. Cabergoline has a stronger affinity for the D2R receptor and longer half-life than L-Dopa, leading to lactotroph apoptosis, tumor shrinkage, and rapid and maintained normalization of PRL levels, with a better side-effect profile. Patients with DHPR deficiency need to be actively monitored for symptomatic hyperprolactinemia, as L-Dopa monotherapy is insufficient to suppress PRL secretion, leading to lactotroph hypertrophy and proliferation over time and development of prolactinomas in later life.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
