A simplified approach to discriminate between healthy subjects and patients with heart failure using cardiac magnetic resonance myocardial deformation imaging.
Undine Ella Witt, Maximilian Leo Müller, Rebecca Elisabeth Beyer, Johannes Wieditz, Susanna Salem, Djawid Hashemi, Wensu Chen, Mina Cvetkovic, Anna Clara Nolden, Patrick Doeblin, Moritz Blum, Gisela Thiede, Alexander Huppertz, Henning Steen, Bjoern Andrew Remppis, Volkmar Falk, Tim Friede, Sebastian Kelle
{"title":"A simplified approach to discriminate between healthy subjects and patients with heart failure using cardiac magnetic resonance myocardial deformation imaging.","authors":"Undine Ella Witt, Maximilian Leo Müller, Rebecca Elisabeth Beyer, Johannes Wieditz, Susanna Salem, Djawid Hashemi, Wensu Chen, Mina Cvetkovic, Anna Clara Nolden, Patrick Doeblin, Moritz Blum, Gisela Thiede, Alexander Huppertz, Henning Steen, Bjoern Andrew Remppis, Volkmar Falk, Tim Friede, Sebastian Kelle","doi":"10.1093/ehjimp/qyae093","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Left ventricular global longitudinal strain (LV-GLS) shows promise as a marker to detect early heart failure (HF). This study sought to (i) establish cardiac magnetic resonance imaging (CMR)-derived LV-GLS cut-offs to differentiate healthy from HF for both acquisition-based and post-processing techniques, (ii) assess agreement, and (iii) provide a method to convert LV-GLS between both techniques.</p><p><strong>Methods and results: </strong>A secondary analysis of a prospective study enrolling healthy subjects (<i>n</i> = 19) and HF patients (<i>n</i> = 56) was conducted. LV-GLS was measured using fast strain-encoded imaging (fSENC) and feature tracking (FT). Receiver operating characteristic (ROC) analyses were performed to derive and evaluate LV-GLS cut-offs discriminating between healthy, HF with mild deformation impairment (DI), and HF with severe DI. Linear regression and Bland-Altman analyses assessed agreement. Cut-offs discriminating between healthy and HF were identified at -19.3% and -15.1% for fSENC and FT, respectively. Cut-offs of -15.8% (fSENC) and -10.8% (FT) further distinguished mild from severe DI. No significant differences in area under ROC curve were identified between fSENC and FT. Bland-Altman analysis revealed a bias of -4.01%, 95% CI -4.42, -3.50 for FT, considering fSENC as reference. Linear regression suggested a factor of 0.76 to rescale fSENC-derived LV-GLS to FT. Using this factor on fSENC-derived cut-offs yielded rescaled FT LV-GLS cut-offs of -14.7% (healthy vs. HF) and -12% (mild vs. severe DI).</p><p><strong>Conclusion: </strong>LV-GLS distinguishes healthy from HF with high accuracy. Each measurement technique requires distinct cut-offs, but rescaling factors facilitate conversion. An FT-based LV-GLS ≥ -15% simplifies HF detection in clinical routine.</p>","PeriodicalId":94317,"journal":{"name":"European heart journal. Imaging methods and practice","volume":"2 3","pages":"qyae093"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11421468/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Imaging methods and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjimp/qyae093","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Left ventricular global longitudinal strain (LV-GLS) shows promise as a marker to detect early heart failure (HF). This study sought to (i) establish cardiac magnetic resonance imaging (CMR)-derived LV-GLS cut-offs to differentiate healthy from HF for both acquisition-based and post-processing techniques, (ii) assess agreement, and (iii) provide a method to convert LV-GLS between both techniques.
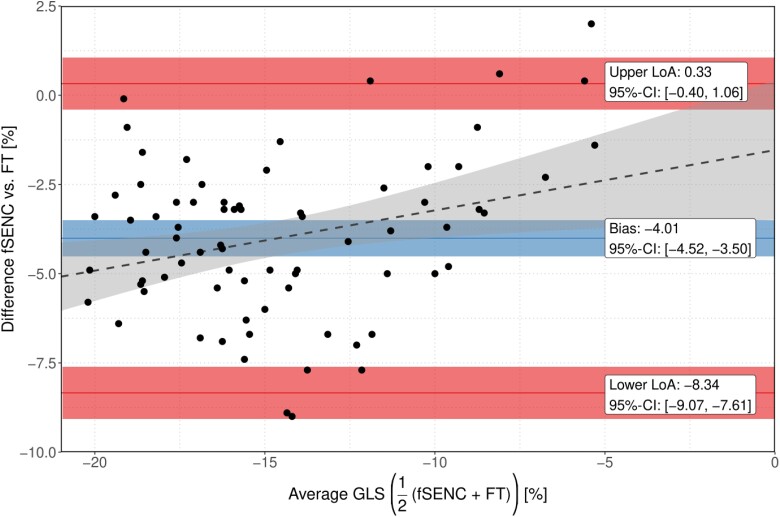
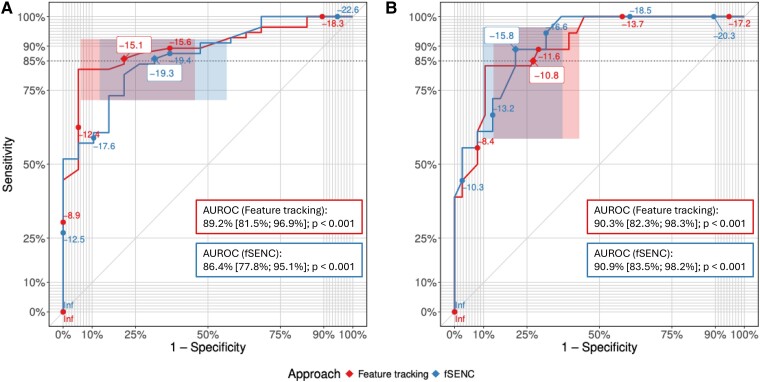
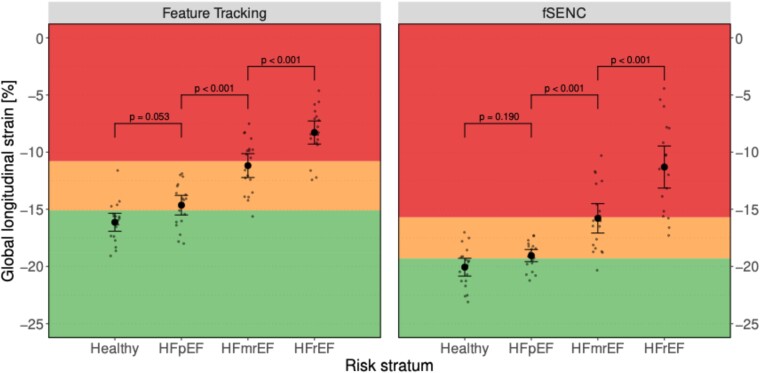
Methods and results: A secondary analysis of a prospective study enrolling healthy subjects (n = 19) and HF patients (n = 56) was conducted. LV-GLS was measured using fast strain-encoded imaging (fSENC) and feature tracking (FT). Receiver operating characteristic (ROC) analyses were performed to derive and evaluate LV-GLS cut-offs discriminating between healthy, HF with mild deformation impairment (DI), and HF with severe DI. Linear regression and Bland-Altman analyses assessed agreement. Cut-offs discriminating between healthy and HF were identified at -19.3% and -15.1% for fSENC and FT, respectively. Cut-offs of -15.8% (fSENC) and -10.8% (FT) further distinguished mild from severe DI. No significant differences in area under ROC curve were identified between fSENC and FT. Bland-Altman analysis revealed a bias of -4.01%, 95% CI -4.42, -3.50 for FT, considering fSENC as reference. Linear regression suggested a factor of 0.76 to rescale fSENC-derived LV-GLS to FT. Using this factor on fSENC-derived cut-offs yielded rescaled FT LV-GLS cut-offs of -14.7% (healthy vs. HF) and -12% (mild vs. severe DI).
Conclusion: LV-GLS distinguishes healthy from HF with high accuracy. Each measurement technique requires distinct cut-offs, but rescaling factors facilitate conversion. An FT-based LV-GLS ≥ -15% simplifies HF detection in clinical routine.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
