{"title":"Comparison of clinicopathological characteristics, efficacy of neoadjuvant therapy, and prognosis in HER2-low and HER2-ultralow breast cancer.","authors":"Feng Guan, Xianli Ju, Lixia Chen, Jiacai Ren, Xiaokang Ke, Bin Luo, Aoling Huang, Jingping Yuan","doi":"10.1186/s13000-024-01557-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study aims to analyze potential differences in clinicopathology, efficacy of neoadjuvant therapy (NAT), and clinical outcome among HER2-null, HER2-ultralow and HER2-low breast cancers.</p><p><strong>Methods: </strong>Consecutive cases of HER2-negative breast cancer that received NAT were included. They were classified as HER2-null (no staining), HER2-ultralow (incomplete faint staining in ≤ 10% of tumour cells) and HER2-low (HER2-1 + or HER2-2+, in situ hybridisation negative). Subgroup analysis was performed based on the HER2 expression level.</p><p><strong>Results: </strong>Out of 302 patients, 215 (71.19%) were HER2-low, 59 (19.54%) were HER2-ultralow, and 28 (9.27%) were HER2-null. In comparison to the HER2-ultralow group, the HER2-low group exhibited higher expression frequencies of ER (p < 0.001), PR (p < 0.001), and AR (p = 0.004), along with a greater prevalence of the luminal subtype (p < 0.001). The HER2-ultralow group also demonstrated a higher prevalence of lymph node metastasis compared to the HER2-null group (p = 0.026). Varied rates of pathologic complete response (pCR) were observed among the three subgroups: HER2-null, HER2-ultralow, and HER2-low, with rates of 35.71%, 22.03%, and 12.56%, respectively. Only the HER2-low subgroup exhibited a significant difference compared to HER2-null (p = 0.001). Despite variations in pCR rates, the three subgroups exhibited comparable disease-free survival (DFS) (p = 0.571). Importantly, we found HER2-low patients with better treatment response (RCB-0/I) exhibited significantly better DFS than those with significant residual disease (RCB-II/III) (P = 0.036). The overall rate of HER2 immunohistochemical score discordance was 45.24%, mostly driven by the conversion between HER2-0 and HER2-low phenotype. Notably, 32.19% of cases initially classified as HER2-0 phenotype on baseline biopsy were later reclassified as HER2-low after neoadjuvant therapy, and it is noteworthy that 22 out of these cases (78.57%) originally had an HER2-ultralow status in the pretreatment biopsy sample.</p><p><strong>Conclusions: </strong>Our results demonstrate the distinct clinicopathological features of HER2-low and HER2-ultralow breast tumors and confirm that RCB is an effective predictor of prognosis in HER2-low populations for the first time. Notably, our findings demonstrate high instability in both HER2-low and HER2-ultralow expression from the primary baseline biopsy to residual disease after NAT. Furthermore, this study is the first to investigate the clinicopathological feature and the effectiveness of NAT for HER2-ultralow breast cancer.</p>","PeriodicalId":11237,"journal":{"name":"Diagnostic Pathology","volume":"19 1","pages":"131"},"PeriodicalIF":2.3000,"publicationDate":"2024-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11441256/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diagnostic Pathology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13000-024-01557-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PATHOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This study aims to analyze potential differences in clinicopathology, efficacy of neoadjuvant therapy (NAT), and clinical outcome among HER2-null, HER2-ultralow and HER2-low breast cancers.
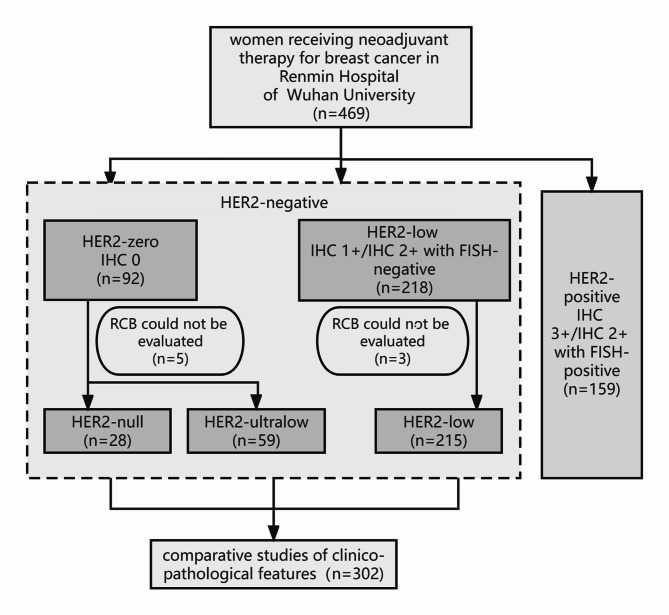
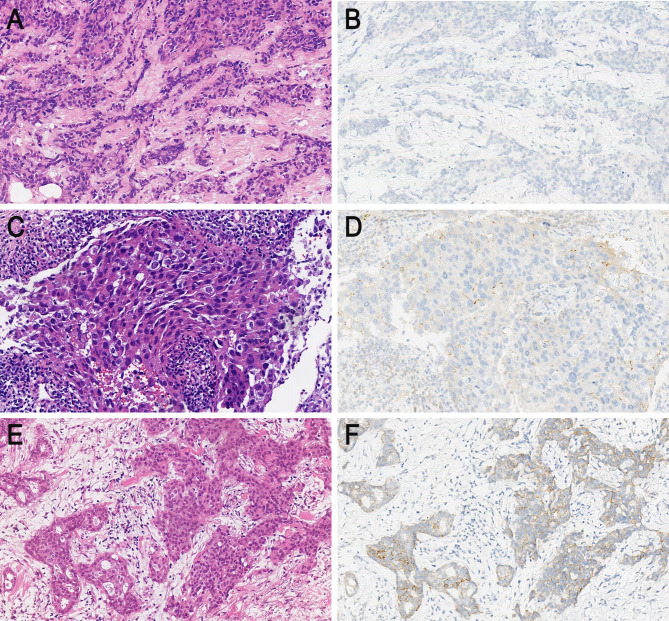
Methods: Consecutive cases of HER2-negative breast cancer that received NAT were included. They were classified as HER2-null (no staining), HER2-ultralow (incomplete faint staining in ≤ 10% of tumour cells) and HER2-low (HER2-1 + or HER2-2+, in situ hybridisation negative). Subgroup analysis was performed based on the HER2 expression level.
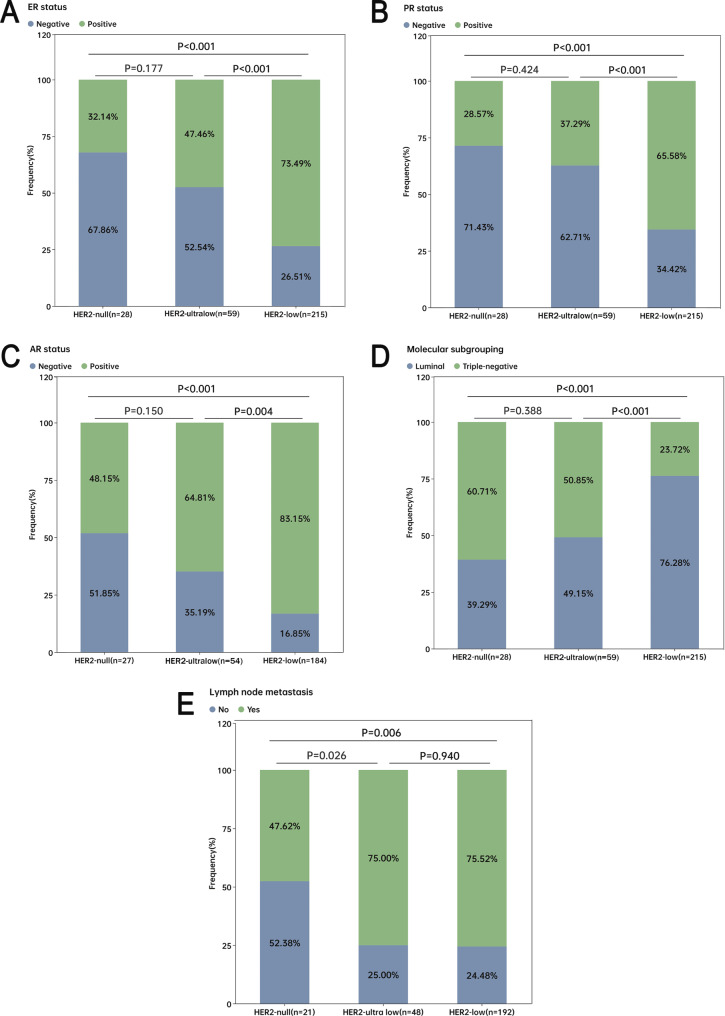
Results: Out of 302 patients, 215 (71.19%) were HER2-low, 59 (19.54%) were HER2-ultralow, and 28 (9.27%) were HER2-null. In comparison to the HER2-ultralow group, the HER2-low group exhibited higher expression frequencies of ER (p < 0.001), PR (p < 0.001), and AR (p = 0.004), along with a greater prevalence of the luminal subtype (p < 0.001). The HER2-ultralow group also demonstrated a higher prevalence of lymph node metastasis compared to the HER2-null group (p = 0.026). Varied rates of pathologic complete response (pCR) were observed among the three subgroups: HER2-null, HER2-ultralow, and HER2-low, with rates of 35.71%, 22.03%, and 12.56%, respectively. Only the HER2-low subgroup exhibited a significant difference compared to HER2-null (p = 0.001). Despite variations in pCR rates, the three subgroups exhibited comparable disease-free survival (DFS) (p = 0.571). Importantly, we found HER2-low patients with better treatment response (RCB-0/I) exhibited significantly better DFS than those with significant residual disease (RCB-II/III) (P = 0.036). The overall rate of HER2 immunohistochemical score discordance was 45.24%, mostly driven by the conversion between HER2-0 and HER2-low phenotype. Notably, 32.19% of cases initially classified as HER2-0 phenotype on baseline biopsy were later reclassified as HER2-low after neoadjuvant therapy, and it is noteworthy that 22 out of these cases (78.57%) originally had an HER2-ultralow status in the pretreatment biopsy sample.
Conclusions: Our results demonstrate the distinct clinicopathological features of HER2-low and HER2-ultralow breast tumors and confirm that RCB is an effective predictor of prognosis in HER2-low populations for the first time. Notably, our findings demonstrate high instability in both HER2-low and HER2-ultralow expression from the primary baseline biopsy to residual disease after NAT. Furthermore, this study is the first to investigate the clinicopathological feature and the effectiveness of NAT for HER2-ultralow breast cancer.
期刊介绍:
Diagnostic Pathology is an open access, peer-reviewed, online journal that considers research in surgical and clinical pathology, immunology, and biology, with a special focus on cutting-edge approaches in diagnostic pathology and tissue-based therapy. The journal covers all aspects of surgical pathology, including classic diagnostic pathology, prognosis-related diagnosis (tumor stages, prognosis markers, such as MIB-percentage, hormone receptors, etc.), and therapy-related findings. The journal also focuses on the technological aspects of pathology, including molecular biology techniques, morphometry aspects (stereology, DNA analysis, syntactic structure analysis), communication aspects (telecommunication, virtual microscopy, virtual pathology institutions, etc.), and electronic education and quality assurance (for example interactive publication, on-line references with automated updating, etc.).




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
