Kristen Burton, Andrew Gold, Peter Abt, Nolan Machado, Kristen Rock, Dmitri Bezinover
{"title":"Making Living-donor Liver Transplantation a Viable Option for Patients With Portopulmonary Hypertension.","authors":"Kristen Burton, Andrew Gold, Peter Abt, Nolan Machado, Kristen Rock, Dmitri Bezinover","doi":"10.1097/TXD.0000000000001710","DOIUrl":null,"url":null,"abstract":"<p><p>Liver transplantation (LT) in patients with significant portopulmonary hypertension (PoPH) is associated with an increased risk of several complications, including graft failure. Graft loss is one of the major reasons. Living donor LT (LDLT) is not routinely performed in the United States in this patient population. In addition, ethical considerations often preclude donation from healthy donors in the setting of a procedure associated with an elevated risk of recipient morbidity and mortality. However, LDLT allows LT to be performed electively, using a superior graft with an improved probability of a good outcome. The key to success in managing these patients is establishing a multidisciplinary team that follows an institutional protocol with clear evaluation and management criteria. These criteria include screening and early diagnosis as well as treatment of PoPH with the goal of optimizing pulmonary arterial hemodynamics and maintaining right ventricular function. Any protocol should include admitting the patient to the hospital a day before surgery for placement of a pulmonary artery catheter to measure and derive relevant hemodynamic variables. A multidisciplinary team should determine the fitness for a transplant a after a careful review of the most up-to-date clinical information. Finally, the team prescribes and executes a plan for optimization and safe perioperative management of the patient. In this report, we discuss our approach to the perioperative management of a patient with significant PoPH who safely underwent LDLT with an excellent postoperative outcome.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"10 10","pages":"e1710"},"PeriodicalIF":1.9000,"publicationDate":"2024-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11427031/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001710","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
Abstract
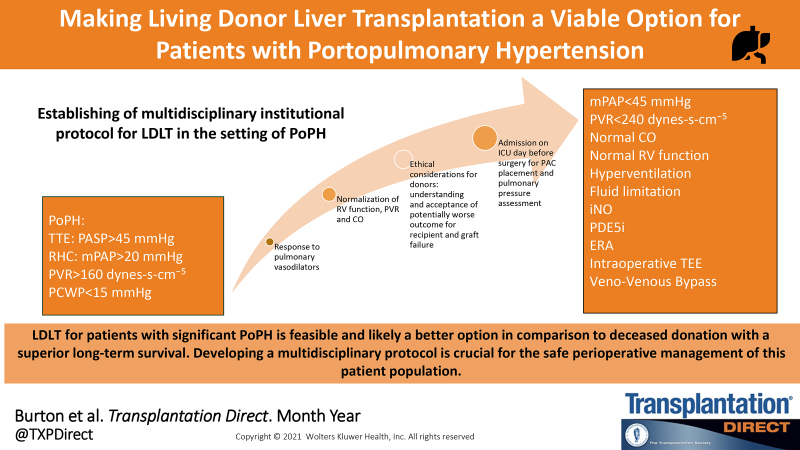
Liver transplantation (LT) in patients with significant portopulmonary hypertension (PoPH) is associated with an increased risk of several complications, including graft failure. Graft loss is one of the major reasons. Living donor LT (LDLT) is not routinely performed in the United States in this patient population. In addition, ethical considerations often preclude donation from healthy donors in the setting of a procedure associated with an elevated risk of recipient morbidity and mortality. However, LDLT allows LT to be performed electively, using a superior graft with an improved probability of a good outcome. The key to success in managing these patients is establishing a multidisciplinary team that follows an institutional protocol with clear evaluation and management criteria. These criteria include screening and early diagnosis as well as treatment of PoPH with the goal of optimizing pulmonary arterial hemodynamics and maintaining right ventricular function. Any protocol should include admitting the patient to the hospital a day before surgery for placement of a pulmonary artery catheter to measure and derive relevant hemodynamic variables. A multidisciplinary team should determine the fitness for a transplant a after a careful review of the most up-to-date clinical information. Finally, the team prescribes and executes a plan for optimization and safe perioperative management of the patient. In this report, we discuss our approach to the perioperative management of a patient with significant PoPH who safely underwent LDLT with an excellent postoperative outcome.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
