Comparing the impact of targeting limited driving pressure to low tidal volume ventilation on mortality in mechanically ventilated adults with COVID-19 ARDS: an exploratory target trial emulation.
Maged Tanios, Ting Ting Wu, Huang Mark Nguyen, Louisa Smith, Raja Mahidhara, John W Devlin
{"title":"Comparing the impact of targeting limited driving pressure to low tidal volume ventilation on mortality in mechanically ventilated adults with COVID-19 ARDS: an exploratory target trial emulation.","authors":"Maged Tanios, Ting Ting Wu, Huang Mark Nguyen, Louisa Smith, Raja Mahidhara, John W Devlin","doi":"10.1136/bmjresp-2024-002439","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>An association between driving pressure (∆P) and the outcomes of invasive mechanical ventilation (IMV) may exist. However, the effect of a sustained limitation of ∆P on mortality in patients with acute respiratory distress syndrome (ARDS), including patients with COVID-19 (COVID-19-related acute respiratory distress syndrome (C-ARDS)) undergoing IMV, has not been rigorously evaluated. The use of emulations of a target trial in intensive care unit research remains in its infancy. To inform future, large ARDS target trials, we explored using a target trial emulation approach to analyse data from a cohort of IMV adults with C-ARDS to determine whether maintaining daily ∆p<15 cm H<sub>2</sub>O (in addition to traditional low tidal volume ventilation (LTVV) (tidal volume 5-7 cc/PBW+plateau pressure (P<sub>plat</sub>) ≤30 cm H<sub>2</sub>O), compared with LTVV alone, affects the 28-day mortality.</p><p><strong>Methods: </strong>To emulate a target trial, adults with C-ARDS requiring >24 hours of IMV were considered to be assigned to limited ∆P or LTVV. Lung mechanics were measured twice daily after ventilator setting adjustments were made. To evaluate the effect of each lung-protective ventilation (LPV) strategy on the 28-day mortality, we fit a stabilised inverse probability weighted marginal structural model that adjusted for baseline and time-varying confounders known to affect protection strategy use/adherence or survival.</p><p><strong>Results: </strong>Among the 92 patients included, 27 (29.3%) followed limited ∆P ventilation, 23 (25.0%) the LTVV strategy and 42 (45.7%) received no LPV strategy. The adjusted estimated 28-day survival was 47.0% (95% CI 23%, 76%) in the limited ∆P group, 70.3% in the LTVV group (95% CI 37.6%, 100%) and 37.6% (95% CI 20.8%, 58.0%) in the no LPV strategy group.</p><p><strong>Interpretation: </strong>Limiting ∆P may not provide additional survival benefits for patients with C-ARDS over LTVV. Our results help inform the development of future target trial emulations focused on evaluating LPV strategies, including reduced ∆P, in adults with ARDS.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"11 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11448172/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2024-002439","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: An association between driving pressure (∆P) and the outcomes of invasive mechanical ventilation (IMV) may exist. However, the effect of a sustained limitation of ∆P on mortality in patients with acute respiratory distress syndrome (ARDS), including patients with COVID-19 (COVID-19-related acute respiratory distress syndrome (C-ARDS)) undergoing IMV, has not been rigorously evaluated. The use of emulations of a target trial in intensive care unit research remains in its infancy. To inform future, large ARDS target trials, we explored using a target trial emulation approach to analyse data from a cohort of IMV adults with C-ARDS to determine whether maintaining daily ∆p<15 cm H2O (in addition to traditional low tidal volume ventilation (LTVV) (tidal volume 5-7 cc/PBW+plateau pressure (Pplat) ≤30 cm H2O), compared with LTVV alone, affects the 28-day mortality.
Methods: To emulate a target trial, adults with C-ARDS requiring >24 hours of IMV were considered to be assigned to limited ∆P or LTVV. Lung mechanics were measured twice daily after ventilator setting adjustments were made. To evaluate the effect of each lung-protective ventilation (LPV) strategy on the 28-day mortality, we fit a stabilised inverse probability weighted marginal structural model that adjusted for baseline and time-varying confounders known to affect protection strategy use/adherence or survival.
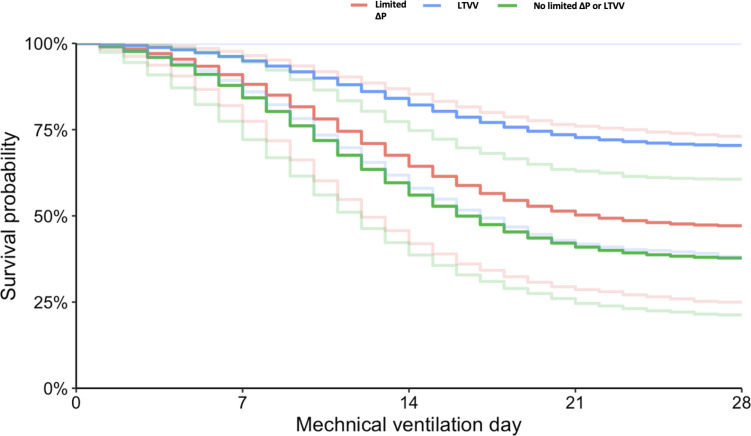
Results: Among the 92 patients included, 27 (29.3%) followed limited ∆P ventilation, 23 (25.0%) the LTVV strategy and 42 (45.7%) received no LPV strategy. The adjusted estimated 28-day survival was 47.0% (95% CI 23%, 76%) in the limited ∆P group, 70.3% in the LTVV group (95% CI 37.6%, 100%) and 37.6% (95% CI 20.8%, 58.0%) in the no LPV strategy group.
Interpretation: Limiting ∆P may not provide additional survival benefits for patients with C-ARDS over LTVV. Our results help inform the development of future target trial emulations focused on evaluating LPV strategies, including reduced ∆P, in adults with ARDS.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
