Meiqi Shi, Ping Chen, Bin Cui, Yuanhu Yao, Juanyi Wang, Tong Zhou, Li Wang
{"title":"Benmelstobart plus anlotinib in patients with EGFR-positive advanced NSCLC after failure of EGFR TKIs therapy: a phase I/II study","authors":"Meiqi Shi, Ping Chen, Bin Cui, Yuanhu Yao, Juanyi Wang, Tong Zhou, Li Wang","doi":"10.1038/s41392-024-01982-2","DOIUrl":null,"url":null,"abstract":"<p>The effect of immune‐based therapies on patients with epidermal growth factor receptor (EGFR)-positive advanced non-small cell lung cancer (NSCLC) resistant to EGFR tyrosine kinase inhibitor (TKI) therapy remains unclear. The ALTER-L038 study aimed to evaluate efficacy and safety of a chemotherapy-free combination of benmelstobart, an anti-programmed cell death ligand 1 antibody, and anlotinib, a small-molecule multi-target anti-angiogenic TKI, in EGFR-positive advanced NSCLC patients who progressed after EGFR TKI therapy. Patients were enrolled in a phase I/II study. In phase I (dose-escalation), patients received anlotinib (8, 10, 12 mg) plus benmelstobart (1200 mg). Recommended phase II dose, determined during phase I, was used in phase II dose-expansion cohort. Primary endpoints were maximum tolerable dose in phase I and progression-free survival (PFS) in phase II. At the data cutoff date (March 10, 2024), 55 patients were enrolled in phase II dose-expansion cohort. Median PFS of patients included in phase II cohort was 9.0 months, median overall survival was 28.9 months, objective response rate was 25.5%, disease control rate was 87.3%, and median duration of response was 19.8 months. Incidence of grade ≥3 treatment-related adverse events in study population was 25.5% (14/55), whereas grade ≥3 immune-related adverse events occurred in 10.9% (6/55) of patients. Benmelstobart plus anlotinib showed promising anti-tumor efficacy with tolerable safety profile, supporting the value of further development of this convenient chemotherapy-free regimen for patients with EGFR-positive advanced NSCLC who progressed after EGFR TKI therapy. Trial Registration: ChiCTR1900026273.</p>","PeriodicalId":21766,"journal":{"name":"Signal Transduction and Targeted Therapy","volume":"24 1","pages":""},"PeriodicalIF":52.7000,"publicationDate":"2024-10-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Signal Transduction and Targeted Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41392-024-01982-2","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
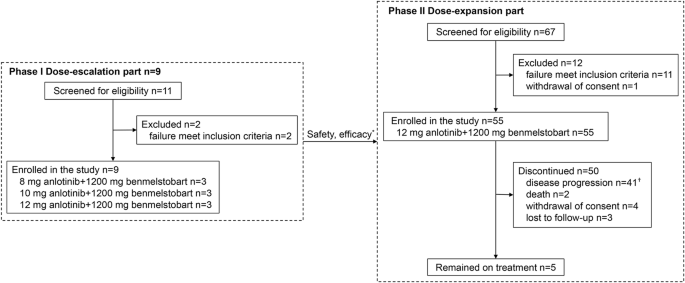
The effect of immune‐based therapies on patients with epidermal growth factor receptor (EGFR)-positive advanced non-small cell lung cancer (NSCLC) resistant to EGFR tyrosine kinase inhibitor (TKI) therapy remains unclear. The ALTER-L038 study aimed to evaluate efficacy and safety of a chemotherapy-free combination of benmelstobart, an anti-programmed cell death ligand 1 antibody, and anlotinib, a small-molecule multi-target anti-angiogenic TKI, in EGFR-positive advanced NSCLC patients who progressed after EGFR TKI therapy. Patients were enrolled in a phase I/II study. In phase I (dose-escalation), patients received anlotinib (8, 10, 12 mg) plus benmelstobart (1200 mg). Recommended phase II dose, determined during phase I, was used in phase II dose-expansion cohort. Primary endpoints were maximum tolerable dose in phase I and progression-free survival (PFS) in phase II. At the data cutoff date (March 10, 2024), 55 patients were enrolled in phase II dose-expansion cohort. Median PFS of patients included in phase II cohort was 9.0 months, median overall survival was 28.9 months, objective response rate was 25.5%, disease control rate was 87.3%, and median duration of response was 19.8 months. Incidence of grade ≥3 treatment-related adverse events in study population was 25.5% (14/55), whereas grade ≥3 immune-related adverse events occurred in 10.9% (6/55) of patients. Benmelstobart plus anlotinib showed promising anti-tumor efficacy with tolerable safety profile, supporting the value of further development of this convenient chemotherapy-free regimen for patients with EGFR-positive advanced NSCLC who progressed after EGFR TKI therapy. Trial Registration: ChiCTR1900026273.
期刊介绍:
Signal Transduction and Targeted Therapy is an open access journal that focuses on timely publication of cutting-edge discoveries and advancements in basic science and clinical research related to signal transduction and targeted therapy.
Scope: The journal covers research on major human diseases, including, but not limited to:
Cancer,Cardiovascular diseases,Autoimmune diseases,Nervous system diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
