{"title":"WEO Newsletter: Tips and Tricks for Endoscopic Ultrasound guided Celiac Plexus interventions","authors":"","doi":"10.1111/den.14935","DOIUrl":null,"url":null,"abstract":"<p>WEO Newsletter Editor: Nalini M Guda MD, MASGE, AGAF, FACG, FJGES</p><p><b>Dr. Sridhar Sundaram</b></p><p><b>MD, DM, FISG</b></p><p>Present Designation:</p><p>Professor (Gastroenterology), Department of Digestive Diseases and Clinical Nutrition, Tata Memorial Hospital, Homi Bhabha National Institute, Mumbai</p><p>Consultant- GI Disease Management Group, Tata Memorial Hospital, Mumbai</p><p>Governing Council Member – Indian Society of Gastroenterology</p><p>Member – ESGE Diversity and Equity Working Group</p><p>Managing Editor – Indian Journal of Gastroenterology</p><p>Member – India EUS Club</p><p>Primary areas of interest: Therapeutic Endoscopic Ultrasound, Endoscopic Resection techniques for early GI cancer</p><p>Abdominal pain due to perineural invasion is one of the most debilitating symptoms associated with pancreaticobiliary cancers. In addition, pain remains one of the most complex symptoms associated with chronic pancreatitis needing intervention (<span>1</span>). Pain from upper abdominal viscera is transmitted via the afferent pathway to the celiac plexus leading into the spinal cord at the T12-L2 level. The efferents from the celiac plexus consists mainly of sympathetic fibres of a network of interconnected para-aortic ganglia, including those at the level of the celiac axis, superior mesenteric artery origin and also renal artery. In addition, parasympathetic efferents of the celiac plexus come from the vagus nerve (<span>2</span>). Traditionally celiac plexus block was performed as an intraoperative ablative procedure. Subsequently fluoroscopy guided celiac plexus interventions were performed. Endoscopic Ultrasound guided celiac plexus block (CPB) was first described in 1996 and has now become the standard of care (<span>3</span>).</p><p>Chronic pancreatitis patients with pain not responding to conventional measures like pancreatic enzyme replacement, antioxidants, non-narcotic and narcotic medications may be candidates who may benefit in short term from CPB. However, the caveat remains that block provides temporary relief and may be an adjunct to other modalities. Celiac plexus neurolysis (CPN) is recommended only in the setting of inoperable pancreatic cancer. In cases of operable pancreatic cancer, neurolysis may lead to scarring the operative field, thereby making surgery technically more challenging. Most patients who do not respond to conventional opioids or require significantly higher doses with adverse events are candidates to consider CPN (<span>4</span>).</p><p>CPB is typically for patients with pain not responding to analgesics and can be repeated at 3–6 months intervals. As pain becomes chronic, response to CPB is likely to be lesser, considering formation of neural feedback loops with cerebral pain conditioning. In patients with pancreatic cancer, pain responds better earlier in the course of disease to CPN. As disease progresses and pain persists, the neural pathways become less responsive and efficacy of CPN reduces (<span>5</span>). Kanno et al showed that EUS CPN does not improve Quality of life and pain compared to those medicated with newer analgesics like Oxycodone and fentanyl (<span>6</span>). Hence EUS CPN may be considered an adjunct in patients needing excessive doses of opioids or having significant adverse effects to opioids.</p><p>Background information on antiplatelets and anticoagulants is important. Aspirin may be continued; however other anticoagulants may need to be titrated. In addition, antibiotic prophylaxis pre-procedure is not recommended. Considering the sympatholytic effect of CPB/CPN leading to hypotension and diarrhea, preloading with 0.5 to 1 L of normal saline is helpful (<span>7</span>). CPB/CPN is done under sedation.</p><p>The celiac plexus is located just below the diaphragm above the origin of the celiac trunk from the aorta. The celiac ganglion is visible in 60–70% cases. Once localized, injection can be done using a 19G or 22G EUS-FNA needle into the plexus or ganglion. After puncture, suction is initially applied to make sure it is not in a vessel. For CPB, 10 ml of 0.25% Bupivacaine and Triamcinolone 40–80 mg (10–40 mg/ml) are injected into the celiac axis. For CPN, in addition to 10 ml of 0.25% Bupivacaine, 10–20 ml of absolute alcohol is also injected into the celiac plexus (<span>4</span>). Injection is known to be associated with clouding above the origin of the celiac axis. Unilateral injection means single injection above the origin of the celiac axis while bilateral injection means injection on both sides of the celiac axis. In a previous systematic review, Puli et al showed that the bilateral technique was associated with higher pain relief than the unilateral technique (84% vs 45%) for both CPB and CPN (<span>8</span>). A subsequent randomized trial by LeBlanc et al with 50 patients showed no significant difference between the unilateral and bilateral technique (69% vs 81%) (<span>9</span>).</p><p>Direct injection into the celiac ganglion was described by Levy et al. and was considered to be safe and effective for pain relief (<span>10</span>). Ascunce et al showed that ability to visualize the celiac ganglion was associated with better response to pain (<span>11</span>). Doi et al. in a randomized controlled trial of 34 patients showed that CGN was associated with higher response rate and higher complete response rate (<span>12</span>). Combination of EUS-CGN with broad plexus neurolysis was associated with higher response rate for pancreatic cancer pain as compared to broad plexus neurolysis (<span>13</span>).</p><p>In a subsequent study, Fujii-Lau et al showed that in 417 patients with pancreatic cancer pain who underwent CPN, survival was lesser in those with CGN than pancreatic cancer controls (193 vs 246 days; HR 1.32) (<span>14</span>). In another randomized trial, Levy et al showed that CPN was associated with higher survival than those who underwent CGN (10.46 months, vs 5.59 months; OR 1.49, p = 0.042), especially those with non-metastatic disease (<span>15</span>). In addition, the concern remains that since all ganglia may not be visible, CGN may have an incomplete effect.</p><p>Another variation is Broad Plexus Neurolysis (BPN) where injection is given above the level of the Superior Mesenteric artery origin leading to more diffuse injection with greater area of neurolysis (<span>16</span>). However, there is lack of large-scale studies backing this practice. It may be an alternative in situations where CPN is ineffective.</p><p>Adverse events are either sedation or procedure related. Transient hypotension due to sympatholytic effect of CPB/CPN is known. Transient diarrhea for 1–2 days is a known complication of CPB/CPN. Transient increase in pain may occur, managed well with narcotic analgesics (<span>17</span>). Rarer complications include bleeding, cardiac complications like arrhythmias, infection with retroperitoneal abscess and also diaphragmatic paralysis.</p><p>Pain relief with CPN is said to be effective in up to 70–80% patients and durable up to 24 months. Patients having metastatic disease and those with direct involvement of celiac plexus by tumor are known to respond poorly. In addition, in case of CPB, previous response to CPB indicates higher likelihood of response to repeat injection (<span>18</span>). In a previous study, heart rate change by >15 beats per min sustained over >30 s was said to be associated with higher response (<span>19</span>). In practice, patients having urge to defecate post-procedure and hypotension intraprocedure suggests likely effective sympatholysis and efficacious CPB/CPN.</p><p>EUS-CPB/CPN remains one of the core interventions performed by endosonologists as an adjunct to medical therapy for managing pain in chronic pancreatitis and pancreatic cancer in a safe and effective manner. While the technique is largely standardized, few variations ensure optimization based on patient and disease related factors. Newer techniques in the form of EUS guided RFA of celiac plexus can be considered in patients who fail conventional EUS CPN.</p><p>Keep in touch! The WEO events calendar</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 10","pages":"1185-1189"},"PeriodicalIF":4.7000,"publicationDate":"2024-10-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14935","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14935","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Professor (Gastroenterology), Department of Digestive Diseases and Clinical Nutrition, Tata Memorial Hospital, Homi Bhabha National Institute, Mumbai
Consultant- GI Disease Management Group, Tata Memorial Hospital, Mumbai
Governing Council Member – Indian Society of Gastroenterology
Member – ESGE Diversity and Equity Working Group
Managing Editor – Indian Journal of Gastroenterology
Member – India EUS Club
Primary areas of interest: Therapeutic Endoscopic Ultrasound, Endoscopic Resection techniques for early GI cancer
Abdominal pain due to perineural invasion is one of the most debilitating symptoms associated with pancreaticobiliary cancers. In addition, pain remains one of the most complex symptoms associated with chronic pancreatitis needing intervention (1). Pain from upper abdominal viscera is transmitted via the afferent pathway to the celiac plexus leading into the spinal cord at the T12-L2 level. The efferents from the celiac plexus consists mainly of sympathetic fibres of a network of interconnected para-aortic ganglia, including those at the level of the celiac axis, superior mesenteric artery origin and also renal artery. In addition, parasympathetic efferents of the celiac plexus come from the vagus nerve (2). Traditionally celiac plexus block was performed as an intraoperative ablative procedure. Subsequently fluoroscopy guided celiac plexus interventions were performed. Endoscopic Ultrasound guided celiac plexus block (CPB) was first described in 1996 and has now become the standard of care (3).
Chronic pancreatitis patients with pain not responding to conventional measures like pancreatic enzyme replacement, antioxidants, non-narcotic and narcotic medications may be candidates who may benefit in short term from CPB. However, the caveat remains that block provides temporary relief and may be an adjunct to other modalities. Celiac plexus neurolysis (CPN) is recommended only in the setting of inoperable pancreatic cancer. In cases of operable pancreatic cancer, neurolysis may lead to scarring the operative field, thereby making surgery technically more challenging. Most patients who do not respond to conventional opioids or require significantly higher doses with adverse events are candidates to consider CPN (4).
CPB is typically for patients with pain not responding to analgesics and can be repeated at 3–6 months intervals. As pain becomes chronic, response to CPB is likely to be lesser, considering formation of neural feedback loops with cerebral pain conditioning. In patients with pancreatic cancer, pain responds better earlier in the course of disease to CPN. As disease progresses and pain persists, the neural pathways become less responsive and efficacy of CPN reduces (5). Kanno et al showed that EUS CPN does not improve Quality of life and pain compared to those medicated with newer analgesics like Oxycodone and fentanyl (6). Hence EUS CPN may be considered an adjunct in patients needing excessive doses of opioids or having significant adverse effects to opioids.
Background information on antiplatelets and anticoagulants is important. Aspirin may be continued; however other anticoagulants may need to be titrated. In addition, antibiotic prophylaxis pre-procedure is not recommended. Considering the sympatholytic effect of CPB/CPN leading to hypotension and diarrhea, preloading with 0.5 to 1 L of normal saline is helpful (7). CPB/CPN is done under sedation.
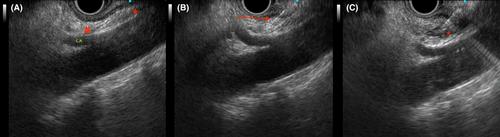
The celiac plexus is located just below the diaphragm above the origin of the celiac trunk from the aorta. The celiac ganglion is visible in 60–70% cases. Once localized, injection can be done using a 19G or 22G EUS-FNA needle into the plexus or ganglion. After puncture, suction is initially applied to make sure it is not in a vessel. For CPB, 10 ml of 0.25% Bupivacaine and Triamcinolone 40–80 mg (10–40 mg/ml) are injected into the celiac axis. For CPN, in addition to 10 ml of 0.25% Bupivacaine, 10–20 ml of absolute alcohol is also injected into the celiac plexus (4). Injection is known to be associated with clouding above the origin of the celiac axis. Unilateral injection means single injection above the origin of the celiac axis while bilateral injection means injection on both sides of the celiac axis. In a previous systematic review, Puli et al showed that the bilateral technique was associated with higher pain relief than the unilateral technique (84% vs 45%) for both CPB and CPN (8). A subsequent randomized trial by LeBlanc et al with 50 patients showed no significant difference between the unilateral and bilateral technique (69% vs 81%) (9).
Direct injection into the celiac ganglion was described by Levy et al. and was considered to be safe and effective for pain relief (10). Ascunce et al showed that ability to visualize the celiac ganglion was associated with better response to pain (11). Doi et al. in a randomized controlled trial of 34 patients showed that CGN was associated with higher response rate and higher complete response rate (12). Combination of EUS-CGN with broad plexus neurolysis was associated with higher response rate for pancreatic cancer pain as compared to broad plexus neurolysis (13).
In a subsequent study, Fujii-Lau et al showed that in 417 patients with pancreatic cancer pain who underwent CPN, survival was lesser in those with CGN than pancreatic cancer controls (193 vs 246 days; HR 1.32) (14). In another randomized trial, Levy et al showed that CPN was associated with higher survival than those who underwent CGN (10.46 months, vs 5.59 months; OR 1.49, p = 0.042), especially those with non-metastatic disease (15). In addition, the concern remains that since all ganglia may not be visible, CGN may have an incomplete effect.
Another variation is Broad Plexus Neurolysis (BPN) where injection is given above the level of the Superior Mesenteric artery origin leading to more diffuse injection with greater area of neurolysis (16). However, there is lack of large-scale studies backing this practice. It may be an alternative in situations where CPN is ineffective.
Adverse events are either sedation or procedure related. Transient hypotension due to sympatholytic effect of CPB/CPN is known. Transient diarrhea for 1–2 days is a known complication of CPB/CPN. Transient increase in pain may occur, managed well with narcotic analgesics (17). Rarer complications include bleeding, cardiac complications like arrhythmias, infection with retroperitoneal abscess and also diaphragmatic paralysis.
Pain relief with CPN is said to be effective in up to 70–80% patients and durable up to 24 months. Patients having metastatic disease and those with direct involvement of celiac plexus by tumor are known to respond poorly. In addition, in case of CPB, previous response to CPB indicates higher likelihood of response to repeat injection (18). In a previous study, heart rate change by >15 beats per min sustained over >30 s was said to be associated with higher response (19). In practice, patients having urge to defecate post-procedure and hypotension intraprocedure suggests likely effective sympatholysis and efficacious CPB/CPN.
EUS-CPB/CPN remains one of the core interventions performed by endosonologists as an adjunct to medical therapy for managing pain in chronic pancreatitis and pancreatic cancer in a safe and effective manner. While the technique is largely standardized, few variations ensure optimization based on patient and disease related factors. Newer techniques in the form of EUS guided RFA of celiac plexus can be considered in patients who fail conventional EUS CPN.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
