Bert Heyrman, Stef Meers, Sélim Sid, Natalie Put, Koen Theunissen, Koen Van Eygen, Nathan De Beule, Maxime Clauwaert, Helena Maes, Alexander Salembier, Jan Lemmens, Ann Van De Velde, Dominik Selleslag, Jason Bouziotis, Ann De Becker, Sébastien Anguille
{"title":"Real-life data of luspatercept in lower-risk myelodysplastic syndromes advocate new research objectives","authors":"Bert Heyrman, Stef Meers, Sélim Sid, Natalie Put, Koen Theunissen, Koen Van Eygen, Nathan De Beule, Maxime Clauwaert, Helena Maes, Alexander Salembier, Jan Lemmens, Ann Van De Velde, Dominik Selleslag, Jason Bouziotis, Ann De Becker, Sébastien Anguille","doi":"10.1002/jha2.1027","DOIUrl":null,"url":null,"abstract":"<p>Myelodysplastic syndromes (MDS) are characterized by ineffective haematopoiesis and a variable risk of progression to acute myeloid leukaemia (AML) [<span>1</span>]. Treatment options are limited and eventually most patients become transfusion-dependent. Transfusion dependency is associated with a decreased quality of life and reduced survival. Transfusion independence (TI) has thus become a primary endpoint in nearly all clinical trials in lower-risk MDS (LR-MDS).</p><p>MDS with ring sideroblasts (MDS-RS), renamed MDS with low blasts and SF3B1 mutation in the World Health Organization (WHO) 2022 classification, has a more favourable prognosis compared to other subtypes [<span>2, 3</span>]. First-line treatment for anaemia is erythropoiesis-stimulating agents (ESA). ESA has been shown to increase haemoglobin (Hb) by about 60% with an estimated median duration of response of 20 months [<span>4</span>]. The increase in Hb correlates with a positive effect on quality of life [<span>5</span>]. Patients with MDS-RS who are transfusion dependent and failed first-line ESA or who are unlikely to respond to ESA (baseline EPO level >200 IU/L) can be treated with luspatercept, a first-in-class erythroid maturating agent. In a phase 3 study (MEDALIST trial) TI for a minimum of 8 weeks during the first 24 weeks was observed in 38% of the patients. At 24 weeks, 65.3% continued in the extension phase because of the clinical benefit of luspatercept at that time [<span>6</span>].</p><p>Real-life data of luspatercept so far are limited and response varies from 18% to >90% [<span>7, 8</span>]. The safety profile as reported in the MEDALIST trial was confirmed in real life with fatigue and cardiovascular events being the most frequent adverse events (AEs) [<span>9</span>]. In terms of quality of life (QoL), a secondary endpoint in the MEDALIST trial, luspatercept could not demonstrate any benefit compared to placebo [<span>10</span>].</p><p>We collected Belgian real-life data of patients who started luspatercept from the start of reimbursement (1 August 2021) with data cut-off on 28 November 2023. Data were collected during December 2023 and January 2024. The ethical committee of the University Hospital Antwerp approved a minimum risk protocol that allowed retrospective collection of the data in different centres and analysis of the data.</p><p>Hospital pharmacies of participating centres provided a list of luspatercept-exposed patients. Patients who received luspatercept in the context of a clinical trial or with a follow-up less than 3 months from the first dose administration were excluded. Transfusion burden (TB) was defined as no TB (0 packed cells/8 weeks), low TB (1–4 units of packed cells/8 weeks), intermediate TB (5–7 packed cells/8 weeks) and high TB (> 7 units of packed cells/8 weeks). Erythroid response was defined as a change in the TB category or an increase in Hb level of at least 1.5 g/dL for patients with no TB. We analysed the duration of treatment, the overall survival time since diagnosis, and the time to progression since diagnosis with the Kaplan-Meier method. The analyses were performed with Stata/SE 18.0.</p><p>We collected data on 77 patients, treated in 14 different centres. The median age at the start of luspatercept was 79 years. Patient and disease characteristics are summarized in Table 1. Forty-three out of 77 patients (55.8%) have stopped treatment during the observation window. The median [interquartile range {IQR}] time since diagnosis, based on 75 patients, was 4.61 [2.29; 7.40] years. Disease progression to higher-risk MDS or AML since diagnosis occurred in 11 out of 77 patients (14.3%). We estimated that progression occurs in 25% of patients in 12 years post-diagnosis. Death from any cause (apart from disease progression) was reported in 13%. The probability of surviving at least eight, 4 years after diagnosis was 75%.</p><p>Previous therapies consisted of ESA (70.1%), or ESA in frontline and study drugs in the second (14.3%) or third line (1.3%). All but one patient (who responded to therapy) were diagnosed with MDS-RS. Luspatercept was administered according to the label at a starting dose of 1 mg/kg once every 3 weeks in all patients. Thirty-four patients were still on treatment at the data cut-off, and 43 previously stopped treatment.</p><p>Reasons to stop treatment were AE (16.3%, <i>n</i> = 7 [i.e. fatigue in three, asthenia in one, hypertension in two and discomfort following administration in one]), death (23.3%, <i>n</i> = 10), no response (34.9%, <i>n</i> = 15), disease progression (25.6%, <i>n</i> = 11). All patients who stopped due to no response stopped treatment at the maximum dose of 1.75 mg/kg.</p><p>Seventy-six patients were included in the response analysis of which 65.8% showed a response to treatment. The primary endpoint of the registration study (i.e. TI for a minimum of 8 weeks) was calculated on 65 patients, excluding patients who had no transfusion prior to the start of luspatercept and was reached in 35.4%. The overall median [IQR] duration of treatment was 48.3 [21; 110.3] weeks (23.9 [18; 48] weeks in the non-responding group and 83.1 weeks in the responding group with at least 38 weeks on treatment in 75% of patients) (Figure 1).</p><p>This real-life analysis confirms the beneficial effect of luspatercept on anaemia and TB. Response to treatment was similar as reported during the registration study with an overall response to treatment (i.e. decrease in TB) of 65.8% and 35.4% reaching TI of 8 weeks or more.</p><p>During the collection period, molecular analysis was not reimbursed for patients older than 70 years, preventing understanding of drug efficacy in possible different molecular subsets. Reimbursement has changed in the meantime following the implementation of the WHO 2022 classification.</p><p>Our population was older compared to the study population in the MEDALIST trial (the median age at the start of treatment was 79 versus 71 years in the registration study) [<span>6</span>]. Treatment was stopped due to an AE in 16.3%, which is more than observed during the registration study (8%), confirming the frailty of the treated population in real life. These data encourage us to be even more aware of possible side effects.</p><p>Remarkable is that one patient had an erythroid response (intermediate-TB before to low-TB on treatment) and stopped treatment due to pronounced fatigue that resolved following the stop of luspatercept. This adds to our argument that quality of life is superior to TI as a treatment objective [<span>11</span>]. The gap in real-life data on quality of life remains to be filled [<span>12</span>].</p><p><b>Bert Heyrman</b>: Conceptualization; organization; data registration and writing of the first draft. <b>Stef Meers, Sélim Sid, Natalie Put, Koen Theunissen, Koen Van Neygen, Nathan De Beule, Maxime Clauwaert, Helena Maes, Alexander Salembier, Jan Lemmens, Dominik Selleslag and Sébastien Anguille</b>: Data registration. <b>Jason Bouziotis</b>: Statistical analysis. <b>Ann De Becker, Stef Meers and Sébastien Anguille</b>: Critical revision of the manuscript.</p><p>The authors declare to have no conflicts of interest.</p><p>This study was a collaborative effort of the authors and received no funding.</p><p>The study was approved by the ethical committee of the University Hospital Antwerp as a minimum-risk protocol to collect and analyze retrospective data.</p><p>The authors have confirmed patient consent statement is not needed for this submission</p><p>The authors have confirmed clinical trial registration is not needed for this submission.</p>","PeriodicalId":72883,"journal":{"name":"EJHaem","volume":"5 5","pages":"1096-1099"},"PeriodicalIF":1.2000,"publicationDate":"2024-10-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jha2.1027","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"EJHaem","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jha2.1027","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Myelodysplastic syndromes (MDS) are characterized by ineffective haematopoiesis and a variable risk of progression to acute myeloid leukaemia (AML) [1]. Treatment options are limited and eventually most patients become transfusion-dependent. Transfusion dependency is associated with a decreased quality of life and reduced survival. Transfusion independence (TI) has thus become a primary endpoint in nearly all clinical trials in lower-risk MDS (LR-MDS).
MDS with ring sideroblasts (MDS-RS), renamed MDS with low blasts and SF3B1 mutation in the World Health Organization (WHO) 2022 classification, has a more favourable prognosis compared to other subtypes [2, 3]. First-line treatment for anaemia is erythropoiesis-stimulating agents (ESA). ESA has been shown to increase haemoglobin (Hb) by about 60% with an estimated median duration of response of 20 months [4]. The increase in Hb correlates with a positive effect on quality of life [5]. Patients with MDS-RS who are transfusion dependent and failed first-line ESA or who are unlikely to respond to ESA (baseline EPO level >200 IU/L) can be treated with luspatercept, a first-in-class erythroid maturating agent. In a phase 3 study (MEDALIST trial) TI for a minimum of 8 weeks during the first 24 weeks was observed in 38% of the patients. At 24 weeks, 65.3% continued in the extension phase because of the clinical benefit of luspatercept at that time [6].
Real-life data of luspatercept so far are limited and response varies from 18% to >90% [7, 8]. The safety profile as reported in the MEDALIST trial was confirmed in real life with fatigue and cardiovascular events being the most frequent adverse events (AEs) [9]. In terms of quality of life (QoL), a secondary endpoint in the MEDALIST trial, luspatercept could not demonstrate any benefit compared to placebo [10].
We collected Belgian real-life data of patients who started luspatercept from the start of reimbursement (1 August 2021) with data cut-off on 28 November 2023. Data were collected during December 2023 and January 2024. The ethical committee of the University Hospital Antwerp approved a minimum risk protocol that allowed retrospective collection of the data in different centres and analysis of the data.
Hospital pharmacies of participating centres provided a list of luspatercept-exposed patients. Patients who received luspatercept in the context of a clinical trial or with a follow-up less than 3 months from the first dose administration were excluded. Transfusion burden (TB) was defined as no TB (0 packed cells/8 weeks), low TB (1–4 units of packed cells/8 weeks), intermediate TB (5–7 packed cells/8 weeks) and high TB (> 7 units of packed cells/8 weeks). Erythroid response was defined as a change in the TB category or an increase in Hb level of at least 1.5 g/dL for patients with no TB. We analysed the duration of treatment, the overall survival time since diagnosis, and the time to progression since diagnosis with the Kaplan-Meier method. The analyses were performed with Stata/SE 18.0.
We collected data on 77 patients, treated in 14 different centres. The median age at the start of luspatercept was 79 years. Patient and disease characteristics are summarized in Table 1. Forty-three out of 77 patients (55.8%) have stopped treatment during the observation window. The median [interquartile range {IQR}] time since diagnosis, based on 75 patients, was 4.61 [2.29; 7.40] years. Disease progression to higher-risk MDS or AML since diagnosis occurred in 11 out of 77 patients (14.3%). We estimated that progression occurs in 25% of patients in 12 years post-diagnosis. Death from any cause (apart from disease progression) was reported in 13%. The probability of surviving at least eight, 4 years after diagnosis was 75%.
Previous therapies consisted of ESA (70.1%), or ESA in frontline and study drugs in the second (14.3%) or third line (1.3%). All but one patient (who responded to therapy) were diagnosed with MDS-RS. Luspatercept was administered according to the label at a starting dose of 1 mg/kg once every 3 weeks in all patients. Thirty-four patients were still on treatment at the data cut-off, and 43 previously stopped treatment.
Reasons to stop treatment were AE (16.3%, n = 7 [i.e. fatigue in three, asthenia in one, hypertension in two and discomfort following administration in one]), death (23.3%, n = 10), no response (34.9%, n = 15), disease progression (25.6%, n = 11). All patients who stopped due to no response stopped treatment at the maximum dose of 1.75 mg/kg.
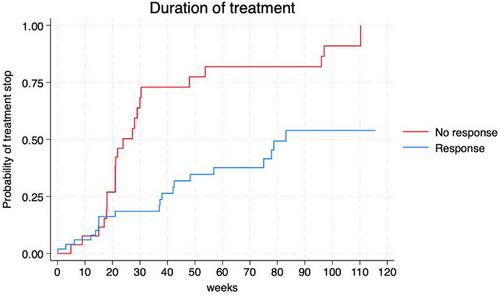
Seventy-six patients were included in the response analysis of which 65.8% showed a response to treatment. The primary endpoint of the registration study (i.e. TI for a minimum of 8 weeks) was calculated on 65 patients, excluding patients who had no transfusion prior to the start of luspatercept and was reached in 35.4%. The overall median [IQR] duration of treatment was 48.3 [21; 110.3] weeks (23.9 [18; 48] weeks in the non-responding group and 83.1 weeks in the responding group with at least 38 weeks on treatment in 75% of patients) (Figure 1).
This real-life analysis confirms the beneficial effect of luspatercept on anaemia and TB. Response to treatment was similar as reported during the registration study with an overall response to treatment (i.e. decrease in TB) of 65.8% and 35.4% reaching TI of 8 weeks or more.
During the collection period, molecular analysis was not reimbursed for patients older than 70 years, preventing understanding of drug efficacy in possible different molecular subsets. Reimbursement has changed in the meantime following the implementation of the WHO 2022 classification.
Our population was older compared to the study population in the MEDALIST trial (the median age at the start of treatment was 79 versus 71 years in the registration study) [6]. Treatment was stopped due to an AE in 16.3%, which is more than observed during the registration study (8%), confirming the frailty of the treated population in real life. These data encourage us to be even more aware of possible side effects.
Remarkable is that one patient had an erythroid response (intermediate-TB before to low-TB on treatment) and stopped treatment due to pronounced fatigue that resolved following the stop of luspatercept. This adds to our argument that quality of life is superior to TI as a treatment objective [11]. The gap in real-life data on quality of life remains to be filled [12].
Bert Heyrman: Conceptualization; organization; data registration and writing of the first draft. Stef Meers, Sélim Sid, Natalie Put, Koen Theunissen, Koen Van Neygen, Nathan De Beule, Maxime Clauwaert, Helena Maes, Alexander Salembier, Jan Lemmens, Dominik Selleslag and Sébastien Anguille: Data registration. Jason Bouziotis: Statistical analysis. Ann De Becker, Stef Meers and Sébastien Anguille: Critical revision of the manuscript.
The authors declare to have no conflicts of interest.
This study was a collaborative effort of the authors and received no funding.
The study was approved by the ethical committee of the University Hospital Antwerp as a minimum-risk protocol to collect and analyze retrospective data.
The authors have confirmed patient consent statement is not needed for this submission
The authors have confirmed clinical trial registration is not needed for this submission.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
