Tulasi Geevar, Yasmeen Abulkhair, Cuihong Wei, Hong Chang
{"title":"Concurrent hyperdiploid acute myeloid leukemia and trisomy 12+ chronic lymphocytic leukemia","authors":"Tulasi Geevar, Yasmeen Abulkhair, Cuihong Wei, Hong Chang","doi":"10.1002/jha2.1009","DOIUrl":null,"url":null,"abstract":"<p>A 75-year-old man presented with weakness and night sweats of 2 weeks duration. He had anemia (75 g/L), and thrombocytopenia (22 × 10<sup>9</sup>/L) with a white blood cell count of 10.6 × 10<sup>9</sup>/L. Peripheral smear (Figure 1, panel A, 10x objective) showed lymphocytosis (7.6 × 10<sup>9</sup>/L) and 8% promonocytes/blasts. Bone marrow aspirate showed 60% blasts/promonocytes and lymphocytosis (panel B, 63x objective). Biopsy (panel C, 20x objective) showed small lymphoid aggregates, positive for CD5/CD20 (panels D&E, 10x objective), and sheets of MPO+/CD117+ blasts (panels F and G, 20x objectives). Flow cytometry (panels I–M) demonstrated ∼40% atypical monocytic cells (green) and ∼25% blasts (red) which were positive for MPO/HLA-DR/CD64/CD117 and negative for CD34/CD14. There were ∼45% lambda restricted B-cells (pink), positive for CD5/CD19/CD20 (dim)/CD23/CD43/CD200. Karyotyping showed 50, XY with trisomy for chromosomes 2, 8, 19, 21, and without structural abnormalities. Next Generation Sequencing showed NRAS mutation with a variant allele frequency of 17%. Fluorescent in situ hybridization (FISH) in addition showed trisomy 12. A diagnosis of concomitant hyperdiploid acute myeloid leukemia (H-AML) and B-chronic lymphocytic leukemia (B-CLL) with trisomy 12 was rendered.</p><p>A custom interphase FISH was performed using probes for chromosomes 8 and 12 (panel H) which showed trisomy 8 (green signals) in larger nuclei and trisomy 12 (red signals) in smaller nuclei. Both abnormalities were not detected within the same nuclei, indicating the different clonal origin of blasts and CLL cells.</p><p>The patient was treated with an induction regimen consisting of 7 days of cytarabin and 3 days of daunorubicin. He entered a hematologic remission for AML, also with a marked reduction in CLL clones in the bone marrow. He completed two cycles of consolidation therapy but relapsed 14 months after treatment, with 25% blasts in the bone marrow. He was started on venetoclax and azacytidine. His disease progressed, and he succumbed to his illness 2 years after the initial diagnosis.</p><p>Hyperdiploidy (≥3 trisomies without structural abnormalities) is a rare event in AML, reported in < 2% of cases, and confers an intermediate prognosis [<span>1</span>]. It is important to distinguish H-AML from AML with complex karyotype (≥3 unrelated chromosome abnormalities in the absence of other recurring genetic abnormalities and excluding hyperdiploidy) as the latter entity has a poor prognosis as per the 2022 ELN recommendations [<span>2, 3</span>]. Trisomy 12 occurs in ∼20% of CLL, associated with intermediate prognosis [<span>4</span>]. The rare concurrence of H-AML and trisomy 12 B-CLL in this case may represent two separate disease processes.</p><p>Tulasi Geevar, Yasmeen Abulkhair, and Cuihong Wei collected data; Tulasi Geevar and Hong Chang wrote the paper; Hong Chang supervised the study.</p><p>The authors declare no conflict of interest.</p><p>The authors received no specific funding for this work.</p><p>The authors have confirmed ethical approval statement is not needed for this submission.</p><p>The authors have confirmed patient consent statement is not needed for this submission.</p><p>The authors have confirmed clinical trial registration is not needed for this submission.</p>","PeriodicalId":72883,"journal":{"name":"EJHaem","volume":"5 5","pages":"1082-1083"},"PeriodicalIF":1.2000,"publicationDate":"2024-09-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jha2.1009","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"EJHaem","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jha2.1009","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
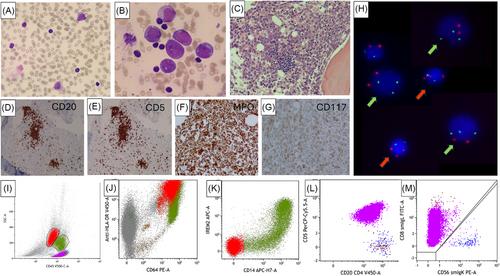
A 75-year-old man presented with weakness and night sweats of 2 weeks duration. He had anemia (75 g/L), and thrombocytopenia (22 × 109/L) with a white blood cell count of 10.6 × 109/L. Peripheral smear (Figure 1, panel A, 10x objective) showed lymphocytosis (7.6 × 109/L) and 8% promonocytes/blasts. Bone marrow aspirate showed 60% blasts/promonocytes and lymphocytosis (panel B, 63x objective). Biopsy (panel C, 20x objective) showed small lymphoid aggregates, positive for CD5/CD20 (panels D&E, 10x objective), and sheets of MPO+/CD117+ blasts (panels F and G, 20x objectives). Flow cytometry (panels I–M) demonstrated ∼40% atypical monocytic cells (green) and ∼25% blasts (red) which were positive for MPO/HLA-DR/CD64/CD117 and negative for CD34/CD14. There were ∼45% lambda restricted B-cells (pink), positive for CD5/CD19/CD20 (dim)/CD23/CD43/CD200. Karyotyping showed 50, XY with trisomy for chromosomes 2, 8, 19, 21, and without structural abnormalities. Next Generation Sequencing showed NRAS mutation with a variant allele frequency of 17%. Fluorescent in situ hybridization (FISH) in addition showed trisomy 12. A diagnosis of concomitant hyperdiploid acute myeloid leukemia (H-AML) and B-chronic lymphocytic leukemia (B-CLL) with trisomy 12 was rendered.
A custom interphase FISH was performed using probes for chromosomes 8 and 12 (panel H) which showed trisomy 8 (green signals) in larger nuclei and trisomy 12 (red signals) in smaller nuclei. Both abnormalities were not detected within the same nuclei, indicating the different clonal origin of blasts and CLL cells.
The patient was treated with an induction regimen consisting of 7 days of cytarabin and 3 days of daunorubicin. He entered a hematologic remission for AML, also with a marked reduction in CLL clones in the bone marrow. He completed two cycles of consolidation therapy but relapsed 14 months after treatment, with 25% blasts in the bone marrow. He was started on venetoclax and azacytidine. His disease progressed, and he succumbed to his illness 2 years after the initial diagnosis.
Hyperdiploidy (≥3 trisomies without structural abnormalities) is a rare event in AML, reported in < 2% of cases, and confers an intermediate prognosis [1]. It is important to distinguish H-AML from AML with complex karyotype (≥3 unrelated chromosome abnormalities in the absence of other recurring genetic abnormalities and excluding hyperdiploidy) as the latter entity has a poor prognosis as per the 2022 ELN recommendations [2, 3]. Trisomy 12 occurs in ∼20% of CLL, associated with intermediate prognosis [4]. The rare concurrence of H-AML and trisomy 12 B-CLL in this case may represent two separate disease processes.
Tulasi Geevar, Yasmeen Abulkhair, and Cuihong Wei collected data; Tulasi Geevar and Hong Chang wrote the paper; Hong Chang supervised the study.
The authors declare no conflict of interest.
The authors received no specific funding for this work.
The authors have confirmed ethical approval statement is not needed for this submission.
The authors have confirmed patient consent statement is not needed for this submission.
The authors have confirmed clinical trial registration is not needed for this submission.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
