{"title":"Circulating plasmablasts in dengue fever","authors":"Robert Noble, Sarah Clifford, Alasdair Duguid","doi":"10.1002/jha2.1011","DOIUrl":null,"url":null,"abstract":"<p>A 31-year-old man presented to the emergency department with a 5-day history of fever, headache and lower back pain which started within 48 h of travelling from his residence in Delhi, India to the United Kingdom. Admission full blood count showed a moderate thrombocytopenia (platelets 76 × 10<sup>9</sup>/L) with otherwise preserved counts (haemoglobin 139 g/L; white cell count 3.8 × 10<sup>9</sup>/L).</p><p>A blood film demonstrated frequent abnormal lymphoid cells, shown above, with deep basophilic cytoplasms, large eccentrically placed nuclei, nucleoli and perinuclear hoff. Immunophenotyping was consistent with a population of plasmablasts; CD19+ CD10− CD20− HLADR+ CD38 (bright) and CD138 (heterogeneous) without surface light chain expression [<span>1</span>].</p><p>The clinical presentation was felt to be in keeping with dengue virus infection which was subsequently confirmed by detecting dengue virus RNA by RT-PCR in conjunction with a positive IgG and indeterminate IgM ELISA. The patient's condition improved with supportive treatment over the following 72 h with resolution of the thrombocytopenia and circulating plasmablasts.</p><p>Dengue is a mosquito-borne viral illness which should be suspected in a febrile traveller from an endemic region displaying suitable clinical features within 2 weeks of last possible exposure [<span>2</span>]. There is a strong association between acute dengue infection and polyclonal plasmablast response. Atypical plasmacytoid cells with severe thrombocytopenia in the returning traveller with fever should alert treating teams to the possibility of dengue virus infection, thereby potentially avoiding further invasive testing for a primary bone marrow pathology (Figure 1, all four panels: circulating plasmablasts present on periphral blood film. M-G-G, x100 objective).</p><p>R. Noble wrote the manuscript. A. Duguid and S. Clifford revised the manuscript.</p><p>The authors declare no conflicts of interest.</p><p>The authors received no specific funding for this work.</p><p>The information presented in this manuscript is deidentified, and there is minimal risk to the patient's privacy or confidentiality.</p><p>No material from other sources is included in this manuscript.</p><p>The authors have confirmed that informed patient consent was obtained.</p><p>Clinical trial registration is not needed for this submission.</p>","PeriodicalId":72883,"journal":{"name":"EJHaem","volume":"5 5","pages":"1080-1081"},"PeriodicalIF":1.2000,"publicationDate":"2024-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jha2.1011","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"EJHaem","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jha2.1011","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
A 31-year-old man presented to the emergency department with a 5-day history of fever, headache and lower back pain which started within 48 h of travelling from his residence in Delhi, India to the United Kingdom. Admission full blood count showed a moderate thrombocytopenia (platelets 76 × 109/L) with otherwise preserved counts (haemoglobin 139 g/L; white cell count 3.8 × 109/L).
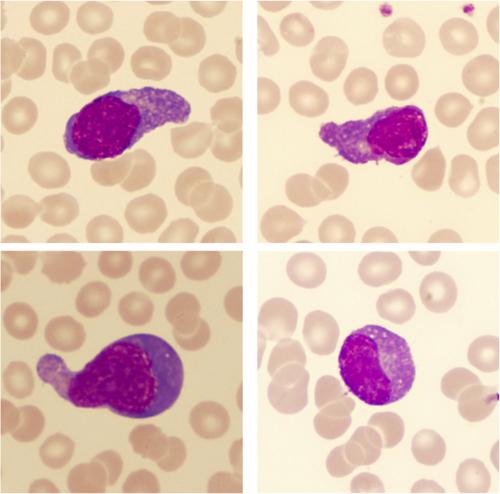
A blood film demonstrated frequent abnormal lymphoid cells, shown above, with deep basophilic cytoplasms, large eccentrically placed nuclei, nucleoli and perinuclear hoff. Immunophenotyping was consistent with a population of plasmablasts; CD19+ CD10− CD20− HLADR+ CD38 (bright) and CD138 (heterogeneous) without surface light chain expression [1].
The clinical presentation was felt to be in keeping with dengue virus infection which was subsequently confirmed by detecting dengue virus RNA by RT-PCR in conjunction with a positive IgG and indeterminate IgM ELISA. The patient's condition improved with supportive treatment over the following 72 h with resolution of the thrombocytopenia and circulating plasmablasts.
Dengue is a mosquito-borne viral illness which should be suspected in a febrile traveller from an endemic region displaying suitable clinical features within 2 weeks of last possible exposure [2]. There is a strong association between acute dengue infection and polyclonal plasmablast response. Atypical plasmacytoid cells with severe thrombocytopenia in the returning traveller with fever should alert treating teams to the possibility of dengue virus infection, thereby potentially avoiding further invasive testing for a primary bone marrow pathology (Figure 1, all four panels: circulating plasmablasts present on periphral blood film. M-G-G, x100 objective).
R. Noble wrote the manuscript. A. Duguid and S. Clifford revised the manuscript.
The authors declare no conflicts of interest.
The authors received no specific funding for this work.
The information presented in this manuscript is deidentified, and there is minimal risk to the patient's privacy or confidentiality.
No material from other sources is included in this manuscript.
The authors have confirmed that informed patient consent was obtained.
Clinical trial registration is not needed for this submission.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
