Videolaryngoscopy vs. direct laryngoscopy for tracheal intubation by experienced anaesthetists: a meta-analysis and trial sequential analysis of randomised controlled trials
Clístenes C. de Carvalho, Idrys H. L. Guedes, Maria V. M. Dantas, Kariem El-Boghdadly
{"title":"Videolaryngoscopy vs. direct laryngoscopy for tracheal intubation by experienced anaesthetists: a meta-analysis and trial sequential analysis of randomised controlled trials","authors":"Clístenes C. de Carvalho, Idrys H. L. Guedes, Maria V. M. Dantas, Kariem El-Boghdadly","doi":"10.1111/anae.16448","DOIUrl":null,"url":null,"abstract":"<p>There is compelling evidence to support the superiority of videolaryngoscopes over direct laryngoscopes for several adult tracheal intubation outcomes [<span>1-3</span>]. However, questions remain regarding this superiority in certain scenarios [<span>4</span>], including whether the results apply to experienced anaesthetists. We aimed to establish whether videolaryngoscopy increases the likelihood of a successful first tracheal intubation attempt and/or reduces the risk of oesophageal intubation and hypoxia when tracheal intubation is attempted by experienced anaesthetists, where high levels of competence with direct laryngoscopes might reduce the advantages of videolaryngoscopes.</p><p>This analysis was based on data from a systematic review, whose protocol was registered prospectively. We included randomised clinical trials that enrolled patients aged ≥ 16 y having elective surgery with tracheal intubation using either videolaryngoscopy or direct laryngoscopy performed by anaesthetists. Studies that involved anaesthesia trainees, anaesthesia associates and medical students were not included. Our primary outcome was rate of first attempt tracheal intubation success. We also assessed rates of oesophageal intubation and hypoxia. A trial sequential analysis was conducted to assess the risk of random error from subsequent meta-analyses for our main outcome.</p><p>In total, we included 120 studies comprising 12,954 patients. The overall risk of bias was generally categorised as either ‘some concerns’ or ‘high’, due primarily to outcome measurement or incomplete reporting (online Supporting Information Figure S1).</p><p>For tracheal intubation first-pass success, we included 117 studies evaluating 12,804 patients. There were varying levels of experience with devices across the studies. Videolaryngoscopy increased the likelihood of success during the first tracheal intubation attempt significantly (relative risk (95%CI) 1.05 (1.02–1.08), p < 0.001, Table 1). The rate of success during a first tracheal intubation attempt was estimated at 90.1% (95%CI 87.7–92.1%) with direct laryngoscopy and 95.3% (93.6–96.6%) with videolaryngoscopy. Further information can be found in the online Supporting Information Figure S2. Publication bias was assessed using the small sample bias approach (online Supporting Information Figure S3), and Egger's test showed a significant asymmetry (p < 0.001). The overall quality of evidence was judged low due to risk of publication bias and inconsistency. Trial sequential analysis indicated that the available data cannot exclude a type 1 error, and thus more information may still be required (Fig. 1).</p><p>For oesophageal intubation, we included 10 studies, with videolaryngoscopy reducing the risk of oesophageal intubation significantly (relative risk (95%CI) 0.33 (0.14–0.76), p = 0.015, Table 1). The quality of the evidence was considered moderate due to imprecision. For hypoxia, we included 10 studies. We did not detect significant differences between videolaryngoscopy and direct laryngoscopy for this outcome (Table 1), and the quality of evidence was low due to relevant imprecision.</p><p>Broadly, our results are consistent with available evidence supporting the superior rate of first-pass tracheal intubation success of videolaryngoscopy compared with direct laryngoscopy [<span>1-3</span>]. Even in scenarios where the value of videolaryngoscopy might be questioned, namely in the hands of experienced clinicians who are already skilled with direct laryngoscopy, these devices still showed a significant increase in the chance of first tracheal intubation attempt success.</p><p>It is important to note the significant variability in study results, highlighting the possibility that the superiority of videolaryngoscopy may not always hold true. Two characteristics that may partially explain this heterogeneity are the diverse types of devices used and the varying levels of expertise with video-assisted devices.</p><p>We must acknowledge the low certainty of the evidence which is due to publication bias and inconsistency. When viewed in isolation, this evidence may not seem robust enough to recommend the routine use of videolaryngoscopes by experienced anaesthetists. However, our results are in keeping with the overall trend, providing additional support for the superior efficacy of videolaryngoscopes over direct laryngoscopes. Therefore, it is reasonable to challenge the scepticism about whether videolaryngoscopy improves outcomes when used by experienced anaesthetists.</p><p>It is logical to assume that if an intervention can improve tracheal intubation efficacy, it would also reduce the risk of complications. As anticipated, our findings indicate that videolaryngoscopy significantly reduces the risk of oesophageal intubation compared with direct laryngoscopy. However, no significant difference was observed between the two interventions regarding incidence of hypoxia. This lack of statistically significant difference does not imply equivalence and may reflect lack of power in our analysis.</p><p>Collectively, the evidence supports the superiority of videolaryngoscopy in improving patient outcomes [<span>1-3</span>]. Even in scenarios where videolaryngoscopes might be deemed less valuable [<span>4</span>], our results still show enhanced efficacy and safety with an increased likelihood of successful first tracheal intubation attempts and a reduced risk of oesophageal intubation. As highlighted elsewhere [<span>1, 5, 6</span>], the focus might shift away from the specific operator towards identifying which video-assisted devices perform best in specific scenarios. However, we acknowledge that further studies are necessary.</p><p>In conclusion, videolaryngoscopy appears to improve tracheal intubation efficacy and safety in adult patients by increasing the chance of first-pass success and reducing the risk of oesophageal intubation during elective procedures performed by experienced anaesthetists, but with moderate or low certainty.</p>","PeriodicalId":7742,"journal":{"name":"Anaesthesia","volume":"79 12","pages":"1371-1373"},"PeriodicalIF":7.5000,"publicationDate":"2024-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/anae.16448","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anaesthesia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/anae.16448","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
There is compelling evidence to support the superiority of videolaryngoscopes over direct laryngoscopes for several adult tracheal intubation outcomes [1-3]. However, questions remain regarding this superiority in certain scenarios [4], including whether the results apply to experienced anaesthetists. We aimed to establish whether videolaryngoscopy increases the likelihood of a successful first tracheal intubation attempt and/or reduces the risk of oesophageal intubation and hypoxia when tracheal intubation is attempted by experienced anaesthetists, where high levels of competence with direct laryngoscopes might reduce the advantages of videolaryngoscopes.
This analysis was based on data from a systematic review, whose protocol was registered prospectively. We included randomised clinical trials that enrolled patients aged ≥ 16 y having elective surgery with tracheal intubation using either videolaryngoscopy or direct laryngoscopy performed by anaesthetists. Studies that involved anaesthesia trainees, anaesthesia associates and medical students were not included. Our primary outcome was rate of first attempt tracheal intubation success. We also assessed rates of oesophageal intubation and hypoxia. A trial sequential analysis was conducted to assess the risk of random error from subsequent meta-analyses for our main outcome.
In total, we included 120 studies comprising 12,954 patients. The overall risk of bias was generally categorised as either ‘some concerns’ or ‘high’, due primarily to outcome measurement or incomplete reporting (online Supporting Information Figure S1).
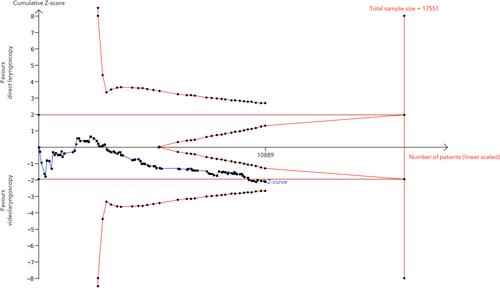
For tracheal intubation first-pass success, we included 117 studies evaluating 12,804 patients. There were varying levels of experience with devices across the studies. Videolaryngoscopy increased the likelihood of success during the first tracheal intubation attempt significantly (relative risk (95%CI) 1.05 (1.02–1.08), p < 0.001, Table 1). The rate of success during a first tracheal intubation attempt was estimated at 90.1% (95%CI 87.7–92.1%) with direct laryngoscopy and 95.3% (93.6–96.6%) with videolaryngoscopy. Further information can be found in the online Supporting Information Figure S2. Publication bias was assessed using the small sample bias approach (online Supporting Information Figure S3), and Egger's test showed a significant asymmetry (p < 0.001). The overall quality of evidence was judged low due to risk of publication bias and inconsistency. Trial sequential analysis indicated that the available data cannot exclude a type 1 error, and thus more information may still be required (Fig. 1).
For oesophageal intubation, we included 10 studies, with videolaryngoscopy reducing the risk of oesophageal intubation significantly (relative risk (95%CI) 0.33 (0.14–0.76), p = 0.015, Table 1). The quality of the evidence was considered moderate due to imprecision. For hypoxia, we included 10 studies. We did not detect significant differences between videolaryngoscopy and direct laryngoscopy for this outcome (Table 1), and the quality of evidence was low due to relevant imprecision.
Broadly, our results are consistent with available evidence supporting the superior rate of first-pass tracheal intubation success of videolaryngoscopy compared with direct laryngoscopy [1-3]. Even in scenarios where the value of videolaryngoscopy might be questioned, namely in the hands of experienced clinicians who are already skilled with direct laryngoscopy, these devices still showed a significant increase in the chance of first tracheal intubation attempt success.
It is important to note the significant variability in study results, highlighting the possibility that the superiority of videolaryngoscopy may not always hold true. Two characteristics that may partially explain this heterogeneity are the diverse types of devices used and the varying levels of expertise with video-assisted devices.
We must acknowledge the low certainty of the evidence which is due to publication bias and inconsistency. When viewed in isolation, this evidence may not seem robust enough to recommend the routine use of videolaryngoscopes by experienced anaesthetists. However, our results are in keeping with the overall trend, providing additional support for the superior efficacy of videolaryngoscopes over direct laryngoscopes. Therefore, it is reasonable to challenge the scepticism about whether videolaryngoscopy improves outcomes when used by experienced anaesthetists.
It is logical to assume that if an intervention can improve tracheal intubation efficacy, it would also reduce the risk of complications. As anticipated, our findings indicate that videolaryngoscopy significantly reduces the risk of oesophageal intubation compared with direct laryngoscopy. However, no significant difference was observed between the two interventions regarding incidence of hypoxia. This lack of statistically significant difference does not imply equivalence and may reflect lack of power in our analysis.
Collectively, the evidence supports the superiority of videolaryngoscopy in improving patient outcomes [1-3]. Even in scenarios where videolaryngoscopes might be deemed less valuable [4], our results still show enhanced efficacy and safety with an increased likelihood of successful first tracheal intubation attempts and a reduced risk of oesophageal intubation. As highlighted elsewhere [1, 5, 6], the focus might shift away from the specific operator towards identifying which video-assisted devices perform best in specific scenarios. However, we acknowledge that further studies are necessary.
In conclusion, videolaryngoscopy appears to improve tracheal intubation efficacy and safety in adult patients by increasing the chance of first-pass success and reducing the risk of oesophageal intubation during elective procedures performed by experienced anaesthetists, but with moderate or low certainty.
期刊介绍:
The official journal of the Association of Anaesthetists is Anaesthesia. It is a comprehensive international publication that covers a wide range of topics. The journal focuses on general and regional anaesthesia, as well as intensive care and pain therapy. It includes original articles that have undergone peer review, covering all aspects of these fields, including research on equipment.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
