Geoffrey P. Dobson, Jodie L. Morris, Hayley L. Letson
{"title":"Traumatic brain injury: Symptoms to systems in the 21st century","authors":"Geoffrey P. Dobson, Jodie L. Morris, Hayley L. Letson","doi":"10.1016/j.brainres.2024.149271","DOIUrl":null,"url":null,"abstract":"<div><div>Severe traumatic brain injury (TBI) is a devastating injury with a mortality of ∼ 25–30 %. Despite decades of high-quality research, no drug therapy has reduced mortality. Why is this so? We argue two contributing factors for the lack of effective drug therapies include the use of specific-pathogen free (SPF) animals for translational research and the flawed practice of single-nodal targeting for drug design. A revolution is required to better understand how the whole body responds to TBI, identify new markers of its progression, and discover new system-acting drugs to treat it. In this review, we present a brief history of TBI, discuss its system’s pathophysiology and propose a new research strategy for the 21st century. TBI progression develops from injury signals radiating from the primary impact, which can cause local ischemia, hemorrhage, excitotoxicity, cellular depolarization, immune dysfunction, sympathetic hyperactivity, blood-brain barrier breach, coagulopathy and whole-body dysfunction. Metabolic reprograming of immune cells drives neuroinflammation and secondary injury processes. We propose if sympathetic hyperactivity and immune cell activation can be corrected early, cardiovascular function and endothelial-glycocalyx-mitochondrial coupling can be restored, and secondary injury minimized with improved patient outcomes. The therapeutic goal is to switch the injury phenotype to a healing phenotype by restoring homeostasis and maintaining sufficient tissue O<sub>2</sub> delivery. We have been developing a small-volume fluid therapy comprising adenosine, lidocaine and magnesium (ALM) to treat TBI and have shown that it blunts the CNS-stress response, supports cardiovascular function and reduces secondary injury. Future research will investigate its suitability for human translation.</div></div>","PeriodicalId":9083,"journal":{"name":"Brain Research","volume":"1845 ","pages":"Article 149271"},"PeriodicalIF":2.6000,"publicationDate":"2024-12-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain Research","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0006899324005250","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/10 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"NEUROSCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
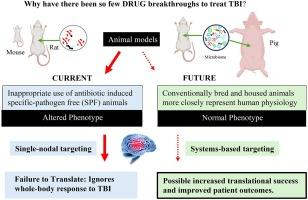
Severe traumatic brain injury (TBI) is a devastating injury with a mortality of ∼ 25–30 %. Despite decades of high-quality research, no drug therapy has reduced mortality. Why is this so? We argue two contributing factors for the lack of effective drug therapies include the use of specific-pathogen free (SPF) animals for translational research and the flawed practice of single-nodal targeting for drug design. A revolution is required to better understand how the whole body responds to TBI, identify new markers of its progression, and discover new system-acting drugs to treat it. In this review, we present a brief history of TBI, discuss its system’s pathophysiology and propose a new research strategy for the 21st century. TBI progression develops from injury signals radiating from the primary impact, which can cause local ischemia, hemorrhage, excitotoxicity, cellular depolarization, immune dysfunction, sympathetic hyperactivity, blood-brain barrier breach, coagulopathy and whole-body dysfunction. Metabolic reprograming of immune cells drives neuroinflammation and secondary injury processes. We propose if sympathetic hyperactivity and immune cell activation can be corrected early, cardiovascular function and endothelial-glycocalyx-mitochondrial coupling can be restored, and secondary injury minimized with improved patient outcomes. The therapeutic goal is to switch the injury phenotype to a healing phenotype by restoring homeostasis and maintaining sufficient tissue O2 delivery. We have been developing a small-volume fluid therapy comprising adenosine, lidocaine and magnesium (ALM) to treat TBI and have shown that it blunts the CNS-stress response, supports cardiovascular function and reduces secondary injury. Future research will investigate its suitability for human translation.
期刊介绍:
An international multidisciplinary journal devoted to fundamental research in the brain sciences.
Brain Research publishes papers reporting interdisciplinary investigations of nervous system structure and function that are of general interest to the international community of neuroscientists. As is evident from the journals name, its scope is broad, ranging from cellular and molecular studies through systems neuroscience, cognition and disease. Invited reviews are also published; suggestions for and inquiries about potential reviews are welcomed.
With the appearance of the final issue of the 2011 subscription, Vol. 67/1-2 (24 June 2011), Brain Research Reviews has ceased publication as a distinct journal separate from Brain Research. Review articles accepted for Brain Research are now published in that journal.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
