{"title":"Association between QT prolongation and cardiovascular mortality in cancer patients.","authors":"Cheng-Han Chan, Chih-Min Liu, Pei-Fen Chen, Li-Lien Liao, I-Chien Wu, Yu-Feng Hu","doi":"10.1186/s40959-024-00271-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cancer patients' vulnerability to QT prolongation contradicts certain anti-cancer drug usage. Until now, the QT prolongation's impact on CV mortality in cancer patients remains unclear, potentially biasing therapeutic decisions.</p><p><strong>Methods: </strong>This retrospective observational cohort included adult cancer patients with an electrocardiogram (ECG) performed in a tertiary hospital in Taiwan. The first performed ECGs after cancer diagnosis (n = 59,568) were analyzed. The corrected QT intervals by Bazett (QTcB), Fridericia (QTcFri), and Framingham (QTcFra) formulae were used to predict the 90-day and one-year CV mortality according to the Taiwan death registry.</p><p><strong>Results: </strong>The AUC of QTcB (90 days: 0.70, 1 year: 0.68) for predicting CV mortality was better than QTcFri and QTcFra (90 days: 0.63 and 0.50, 1 year: 0.65 and 0.56). Using the restricted cubic spline regression model adjusted by age and comorbidities, QTcB increased a significant but trivial risk of CV mortality at 90 days (hazard ratio, 1.007, P = 0.02) and one year (1.006, P < 0.01). Compared to those with QTcB < 500ms, the patients with QTcB ≥ 500ms were older and had more comorbidities and mortalities within one year. The incidence of sudden death and ventricular arrhythmias was only 0.2%. After adjusting for comorbidities, QTcB was neither associated with 90-day nor one-year CV mortality. In the patients already with QTcB ≥ 500ms, the patients receiving the unexpected uses of QT-prolonging drugs were not associated with higher one-year CV mortality than those without (P = 0.14).</p><p><strong>Conclusions: </strong>Rather than a prolonged QT interval per se, comorbidities contributed to CV mortality and irreversible outcomes in cancer patients.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"10 1","pages":"69"},"PeriodicalIF":3.2000,"publicationDate":"2024-10-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11470720/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-024-00271-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cancer patients' vulnerability to QT prolongation contradicts certain anti-cancer drug usage. Until now, the QT prolongation's impact on CV mortality in cancer patients remains unclear, potentially biasing therapeutic decisions.
Methods: This retrospective observational cohort included adult cancer patients with an electrocardiogram (ECG) performed in a tertiary hospital in Taiwan. The first performed ECGs after cancer diagnosis (n = 59,568) were analyzed. The corrected QT intervals by Bazett (QTcB), Fridericia (QTcFri), and Framingham (QTcFra) formulae were used to predict the 90-day and one-year CV mortality according to the Taiwan death registry.
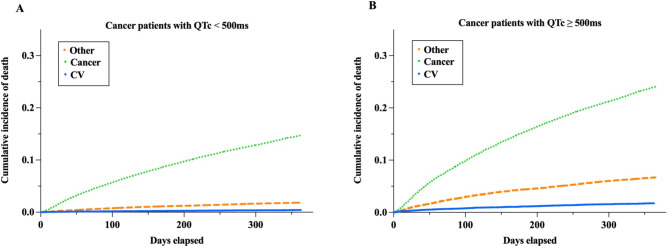
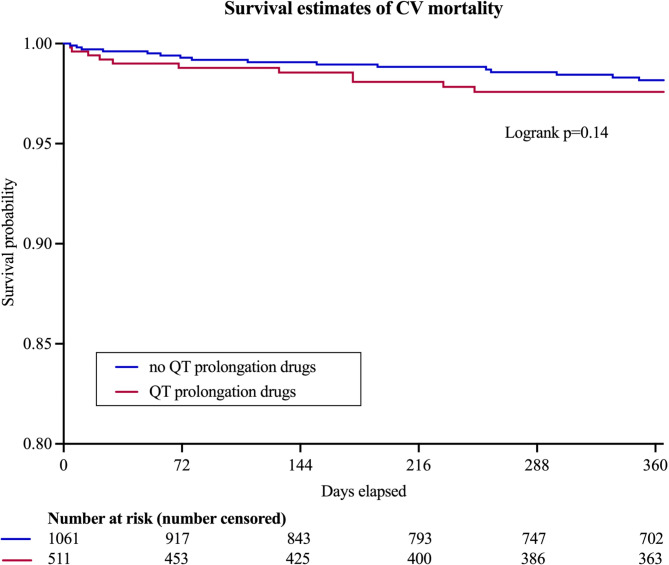
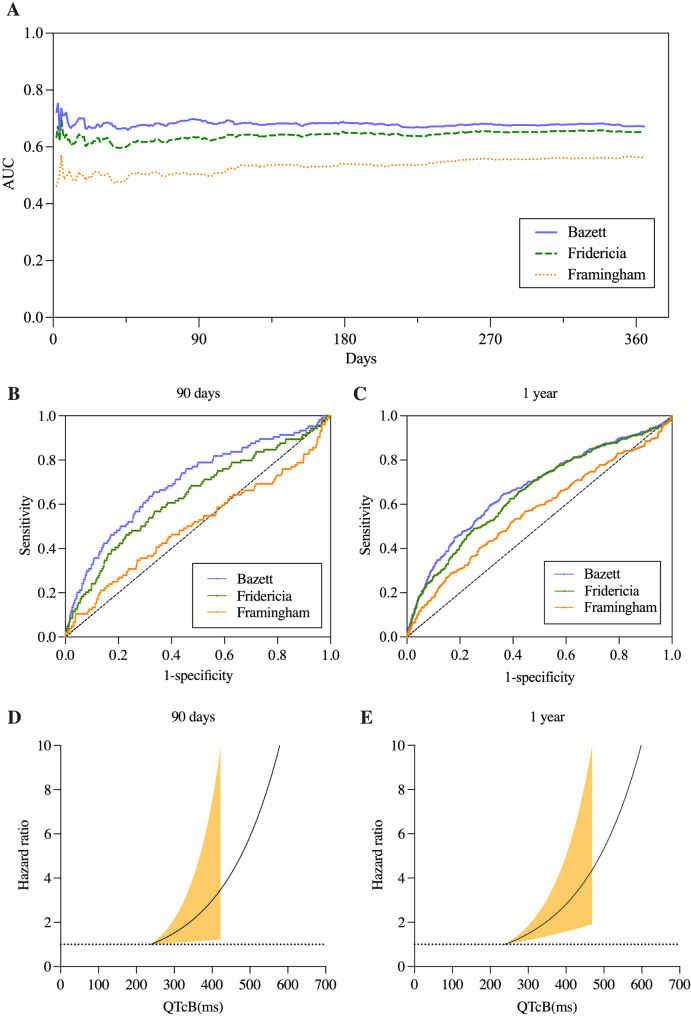
Results: The AUC of QTcB (90 days: 0.70, 1 year: 0.68) for predicting CV mortality was better than QTcFri and QTcFra (90 days: 0.63 and 0.50, 1 year: 0.65 and 0.56). Using the restricted cubic spline regression model adjusted by age and comorbidities, QTcB increased a significant but trivial risk of CV mortality at 90 days (hazard ratio, 1.007, P = 0.02) and one year (1.006, P < 0.01). Compared to those with QTcB < 500ms, the patients with QTcB ≥ 500ms were older and had more comorbidities and mortalities within one year. The incidence of sudden death and ventricular arrhythmias was only 0.2%. After adjusting for comorbidities, QTcB was neither associated with 90-day nor one-year CV mortality. In the patients already with QTcB ≥ 500ms, the patients receiving the unexpected uses of QT-prolonging drugs were not associated with higher one-year CV mortality than those without (P = 0.14).
Conclusions: Rather than a prolonged QT interval per se, comorbidities contributed to CV mortality and irreversible outcomes in cancer patients.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
